- 12 tips in 12 minutes
- Opinionated, illustrated, for early career EPs
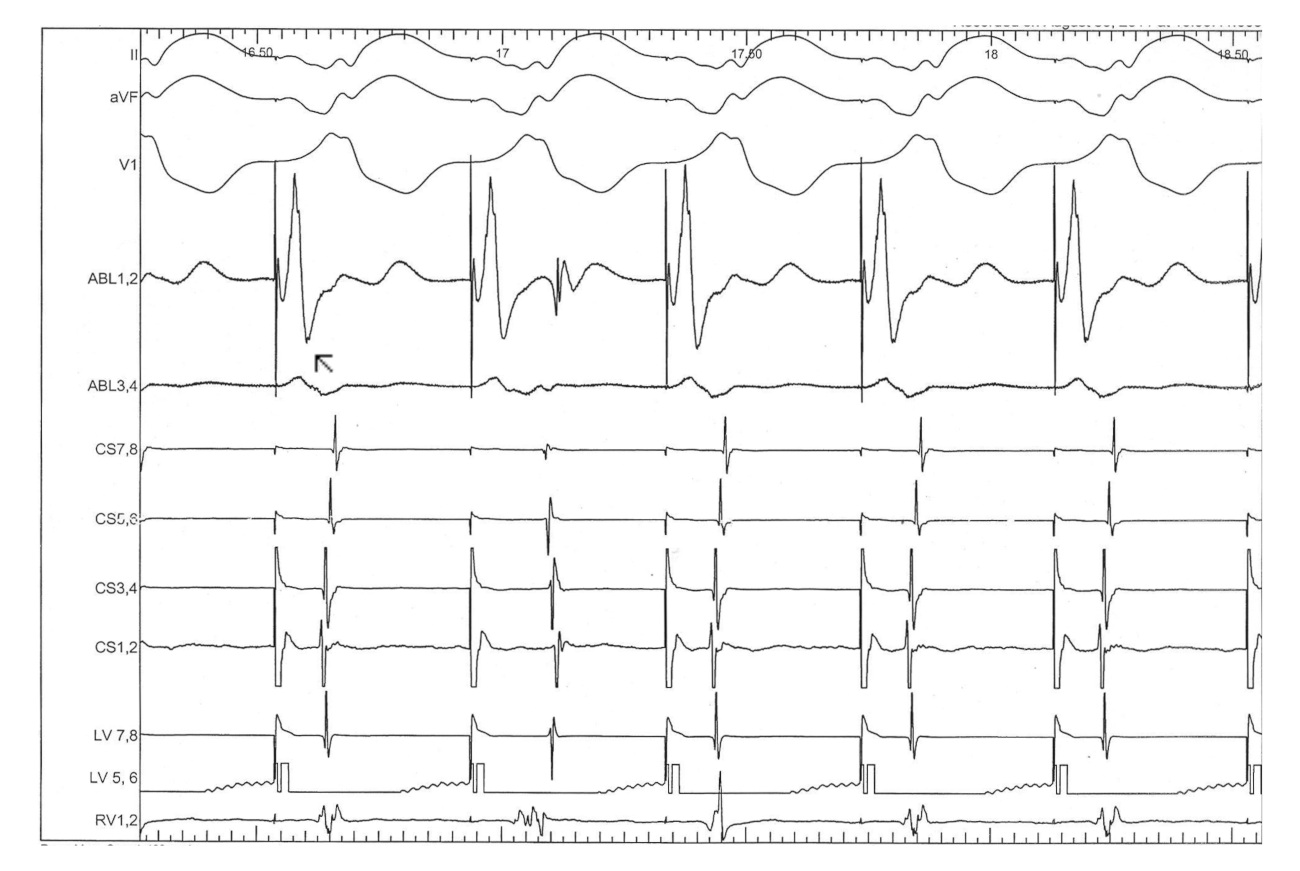
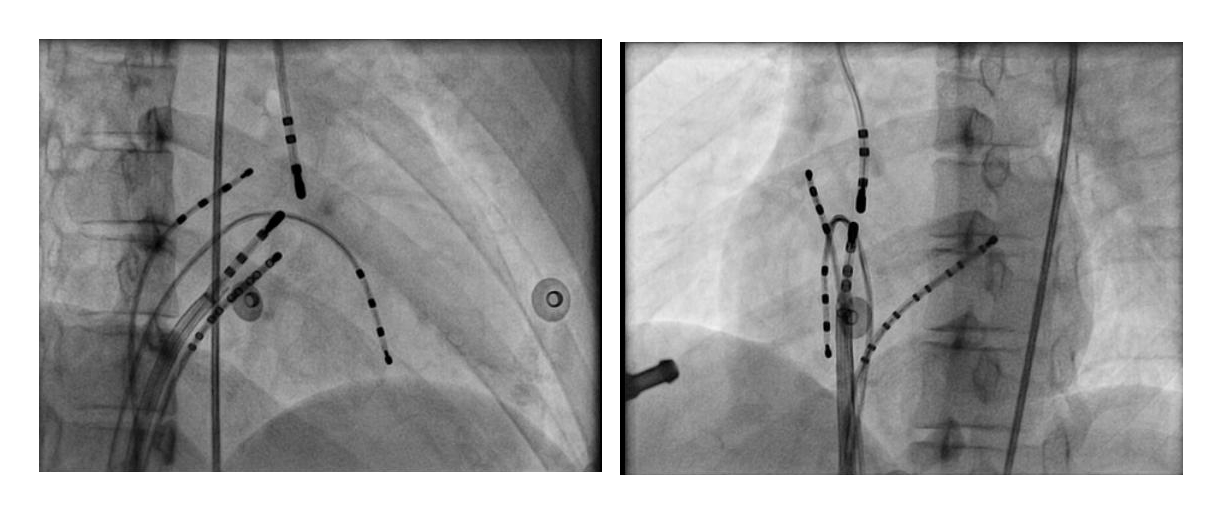
#1 Use four catheters for EP study
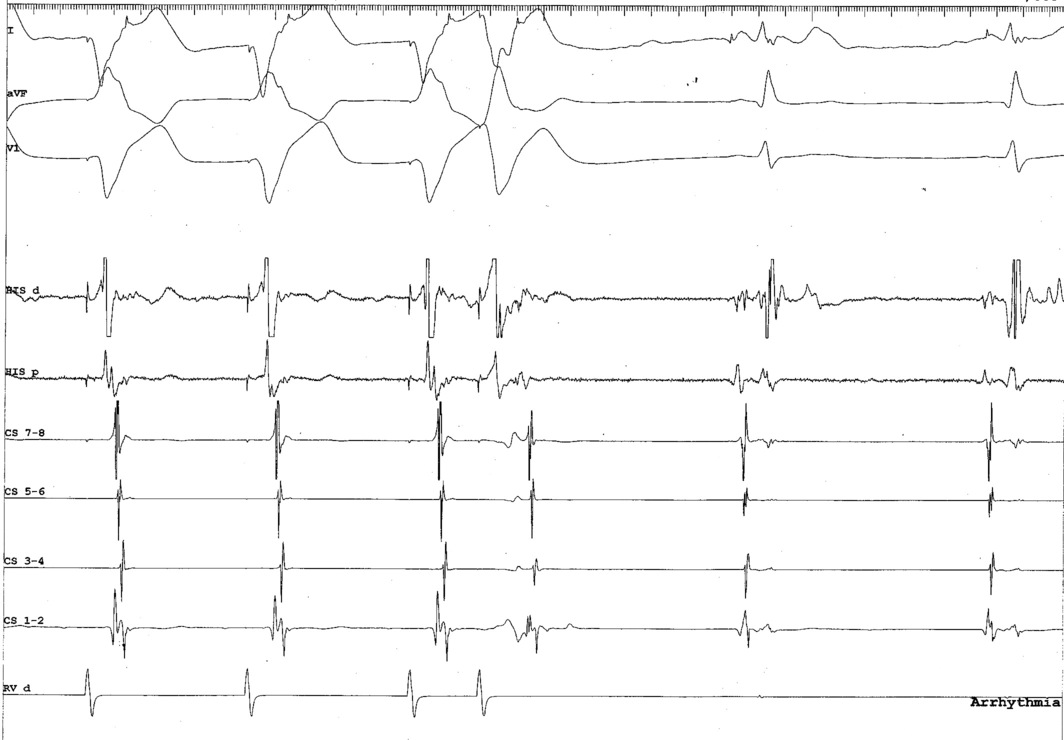
#1 Use four catheters for EP study

But we have an RA catheter And this is clearly a concealed RFW AP
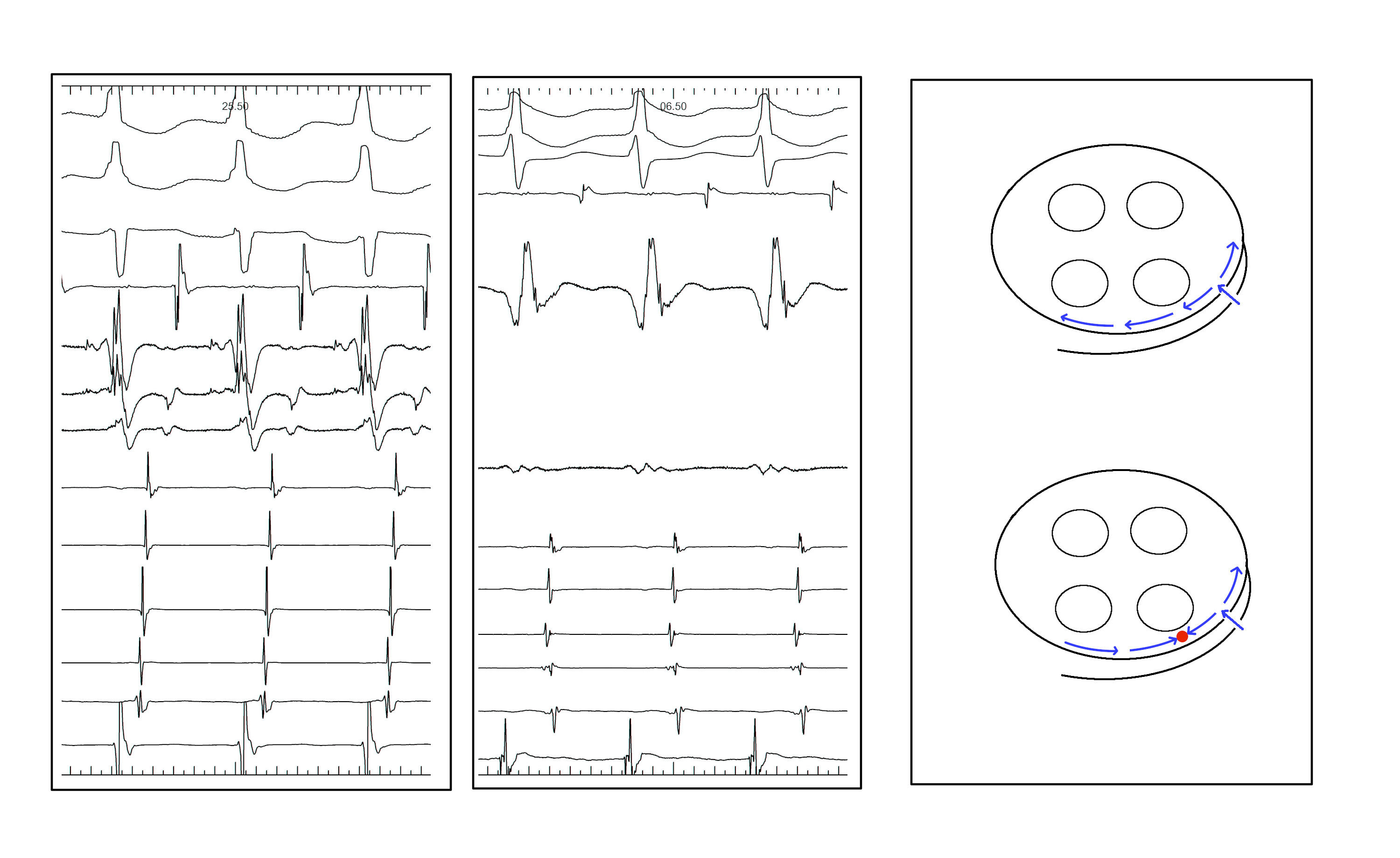
#2 Consider placing the RV catheter at base
#3 Use triggered mode for mapping
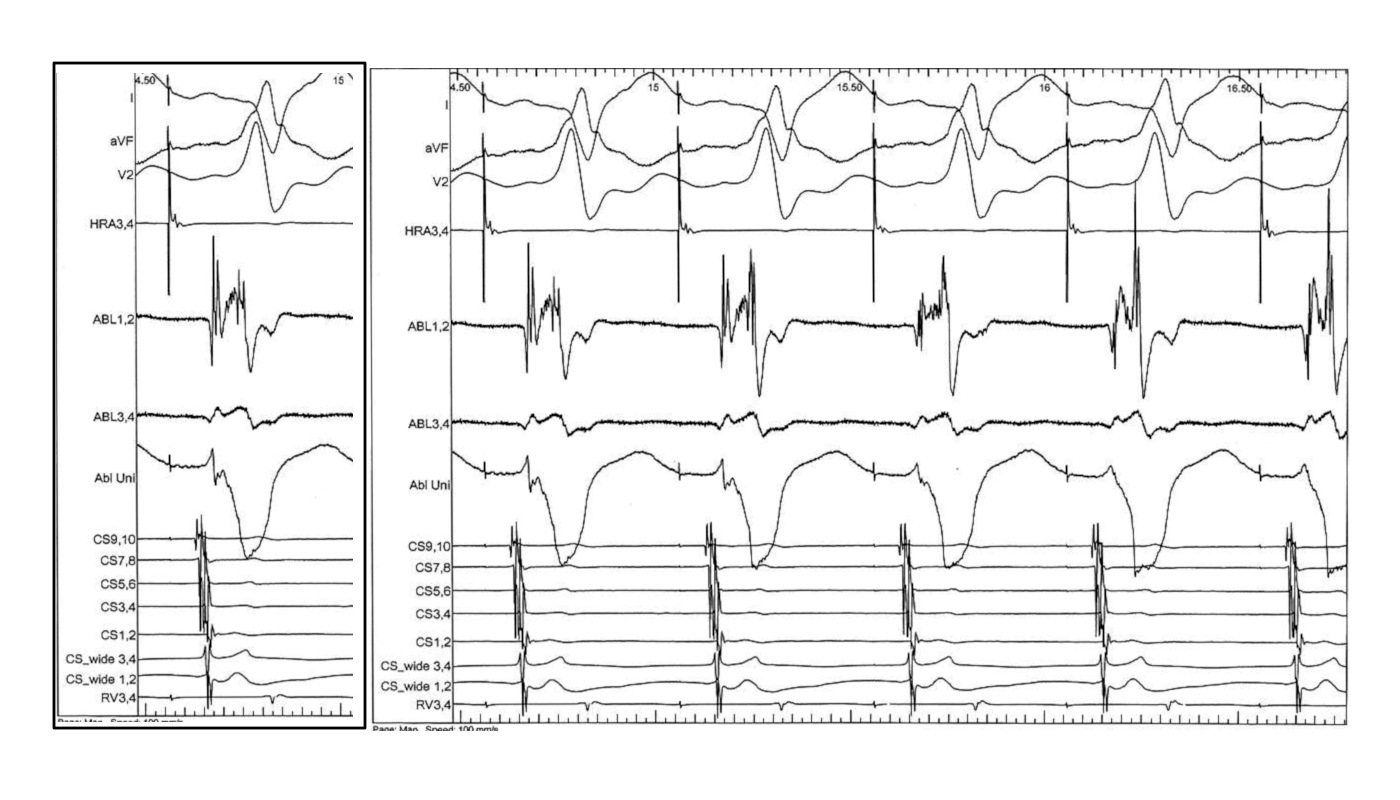
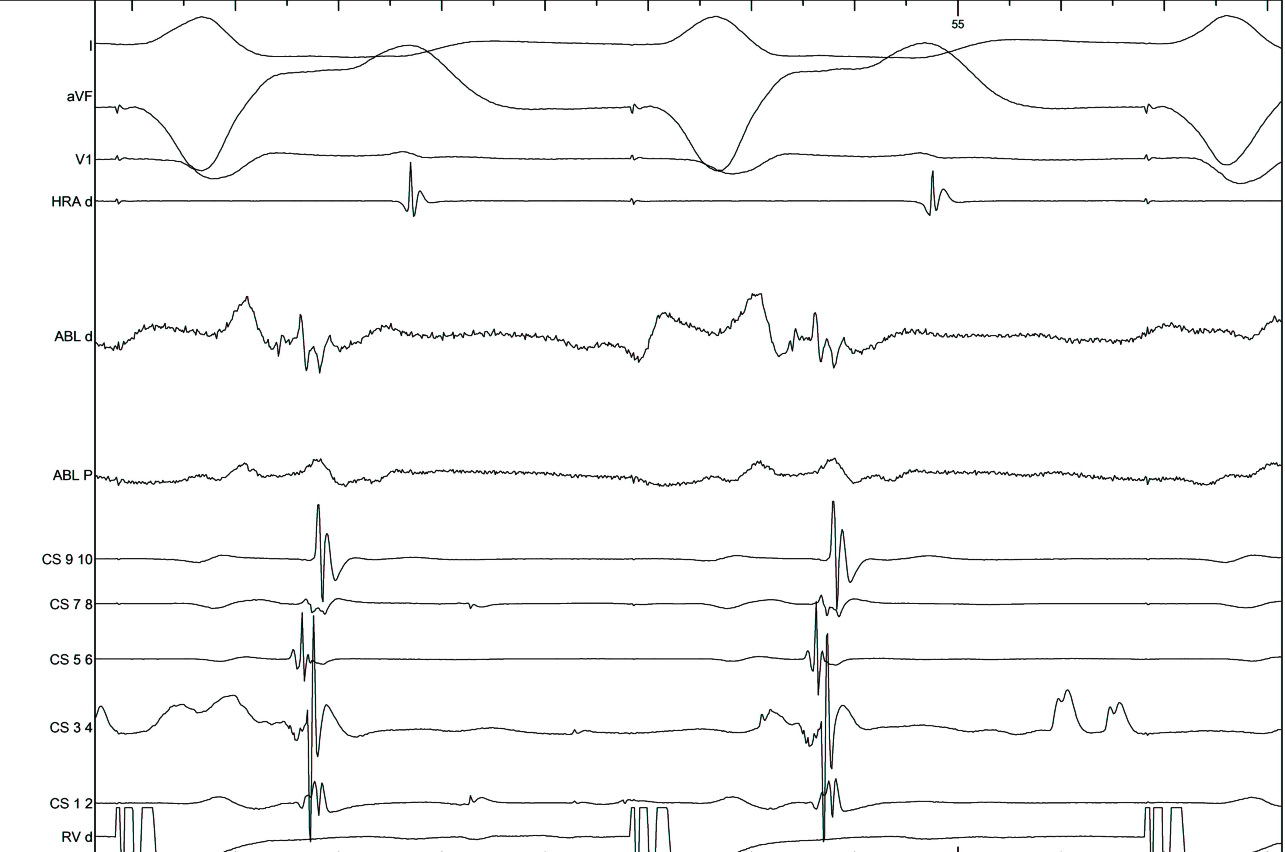
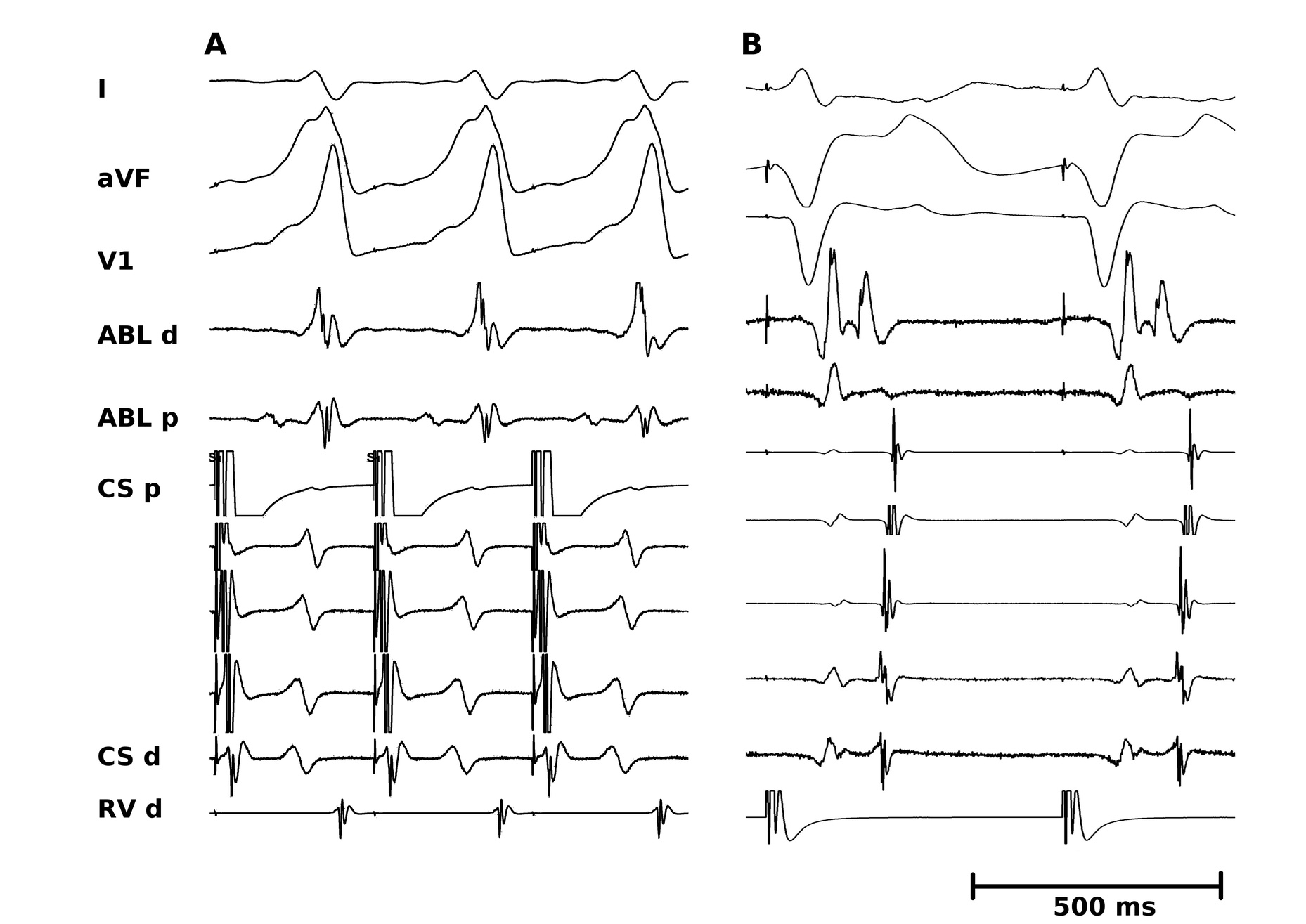
#4 Key to mapping is to identify signal components
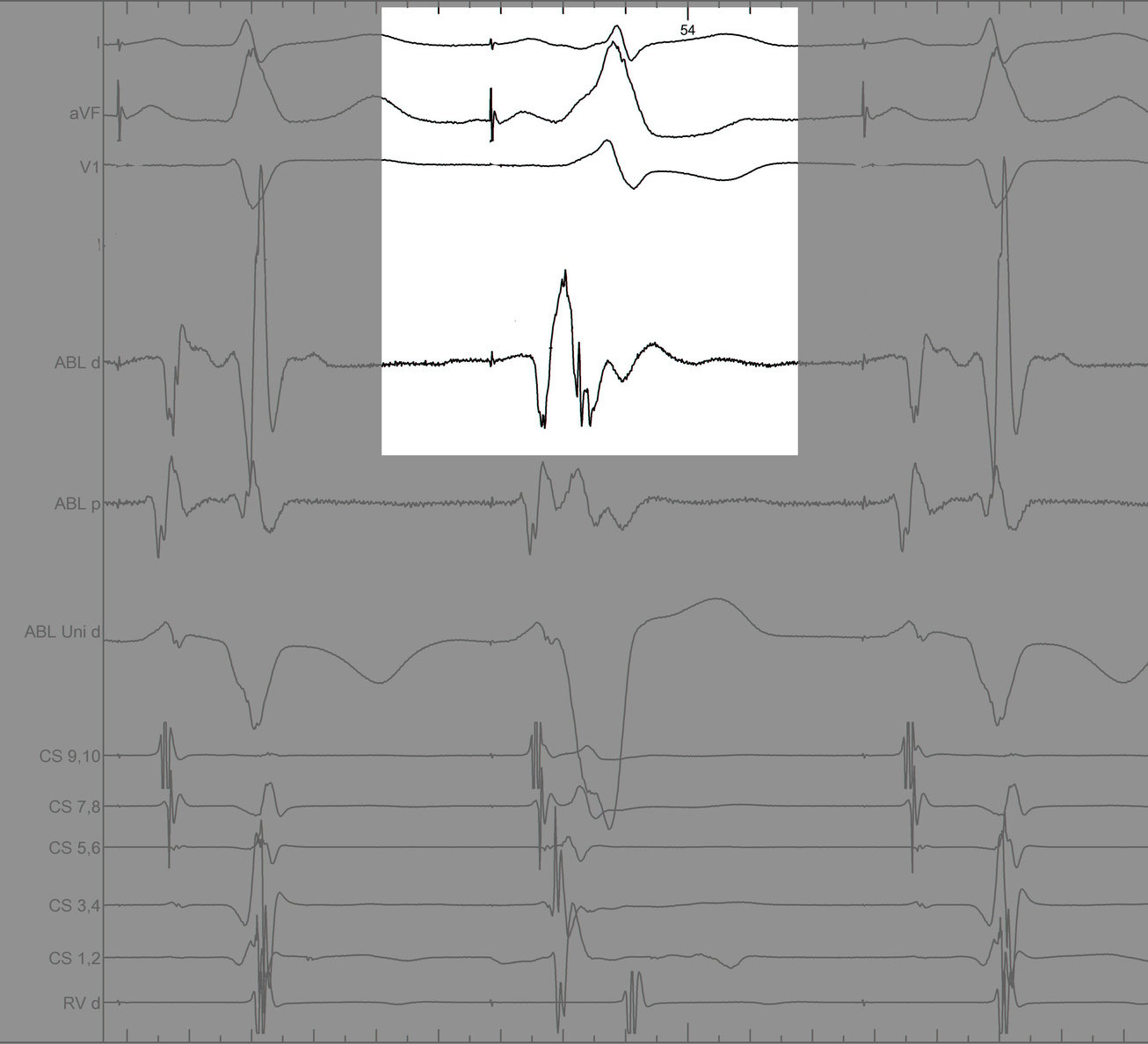
#4 Key to mapping is to identify signal components
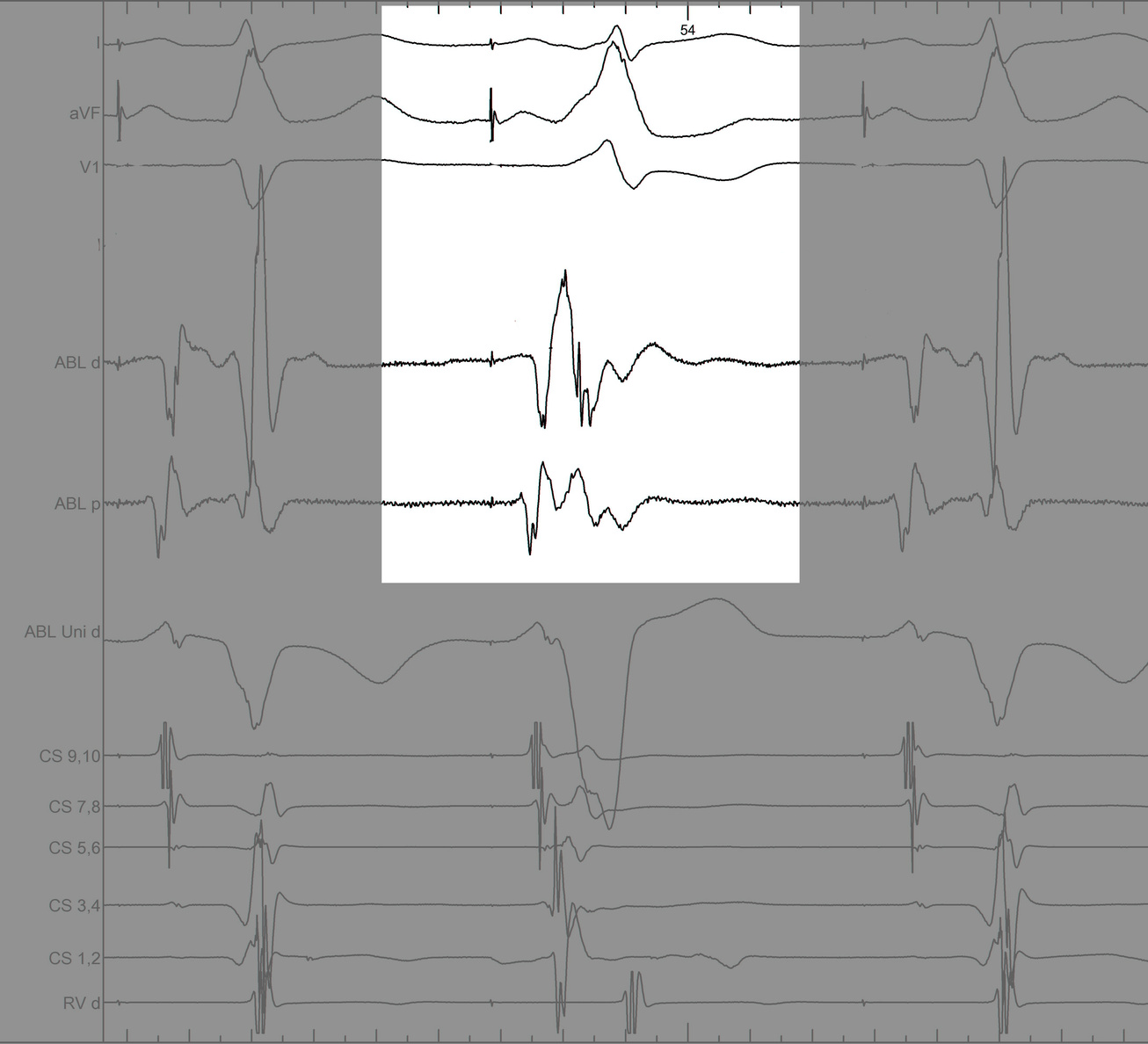
#4 Key to mapping is to identify signal components
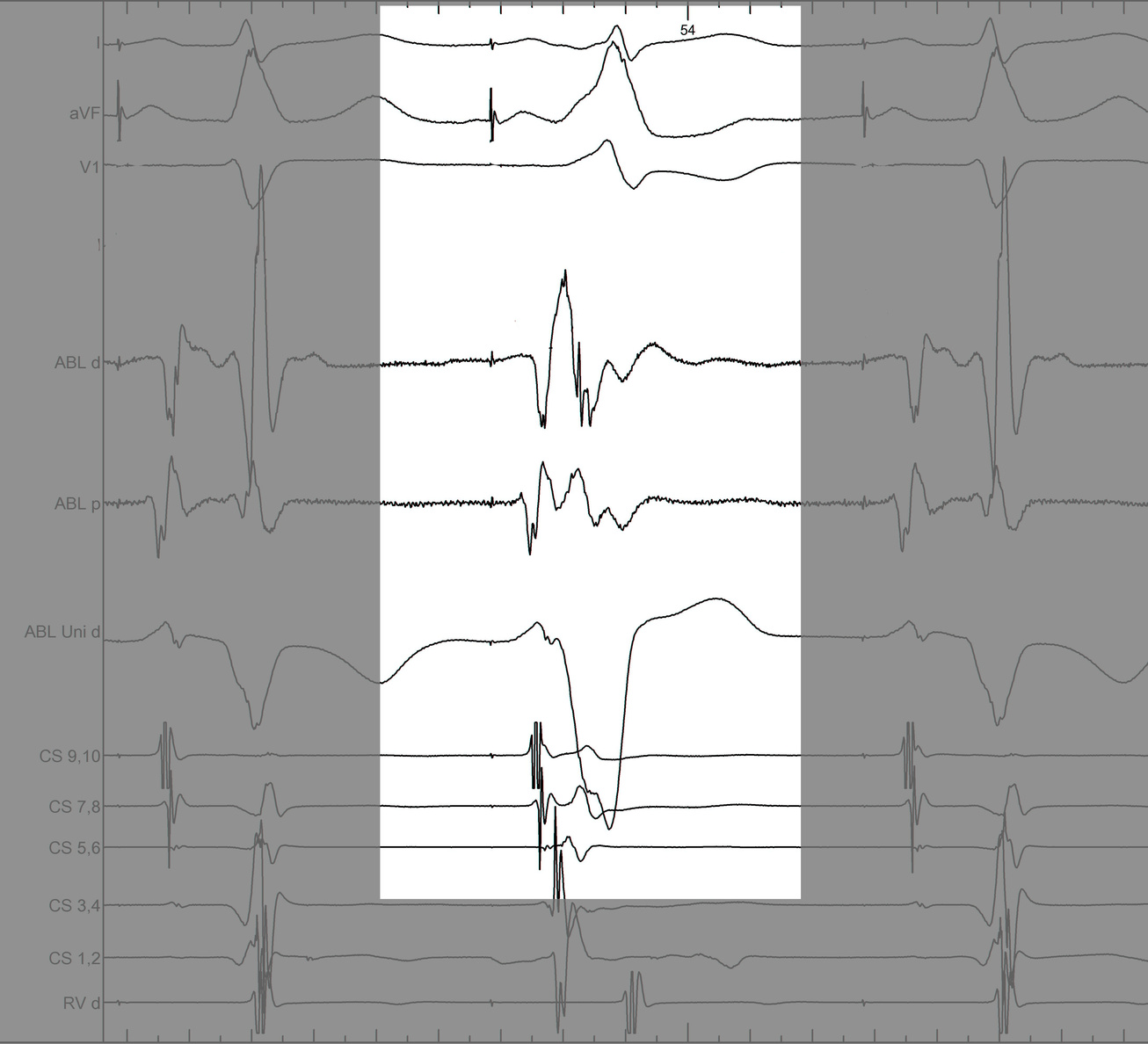
#4 Key to mapping is to identify signal components
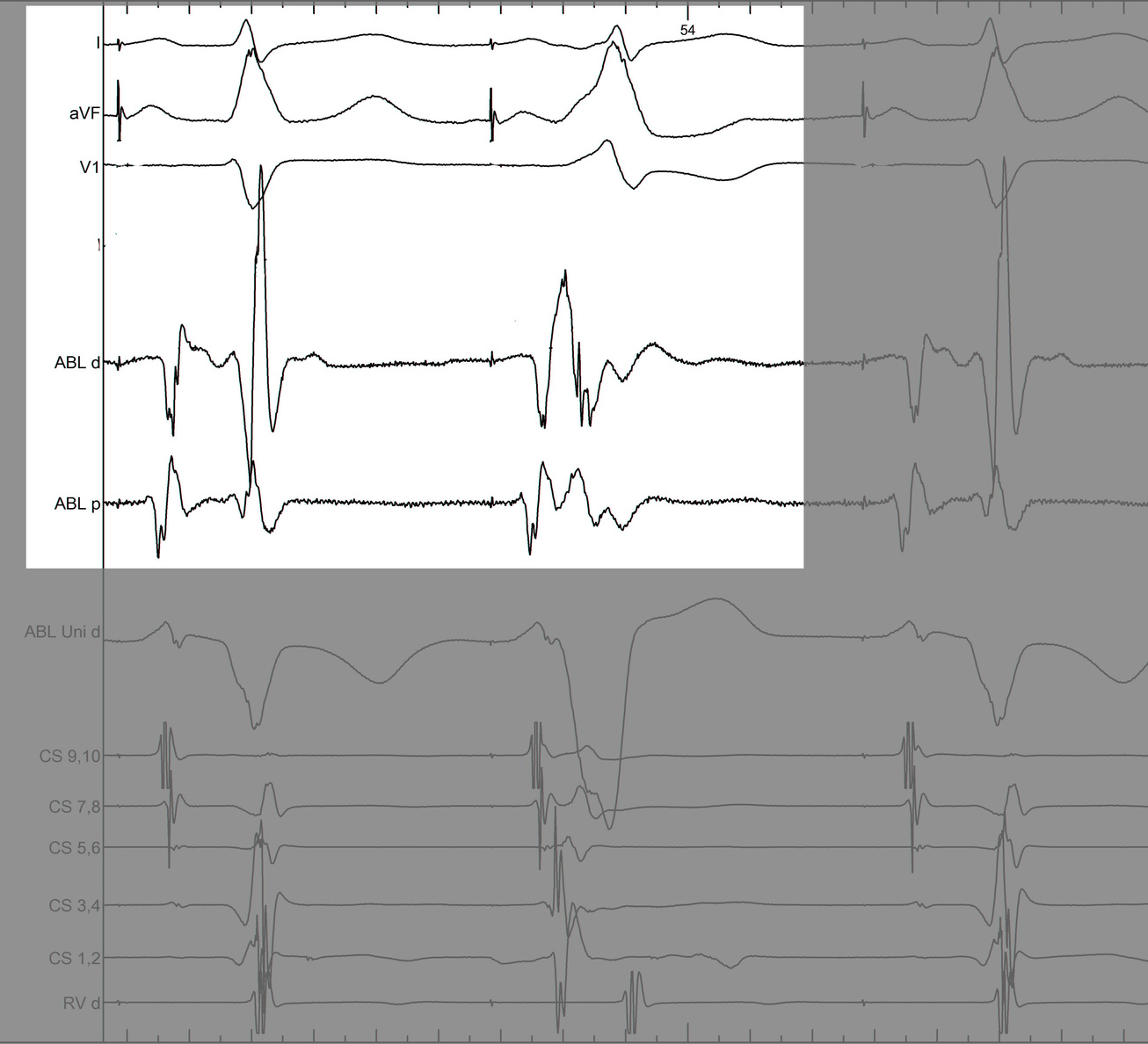
#4 Key to mapping is to identify signal components
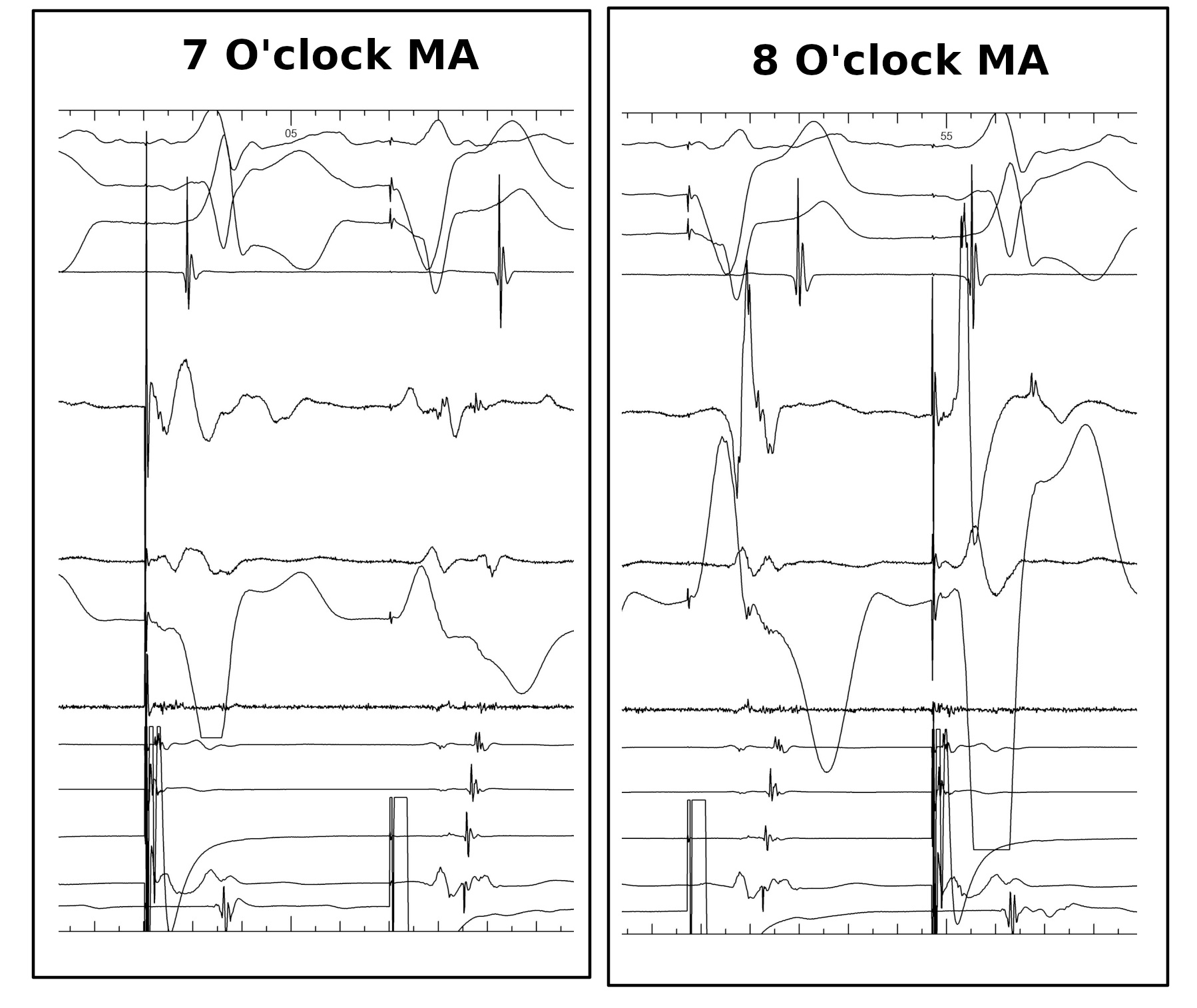
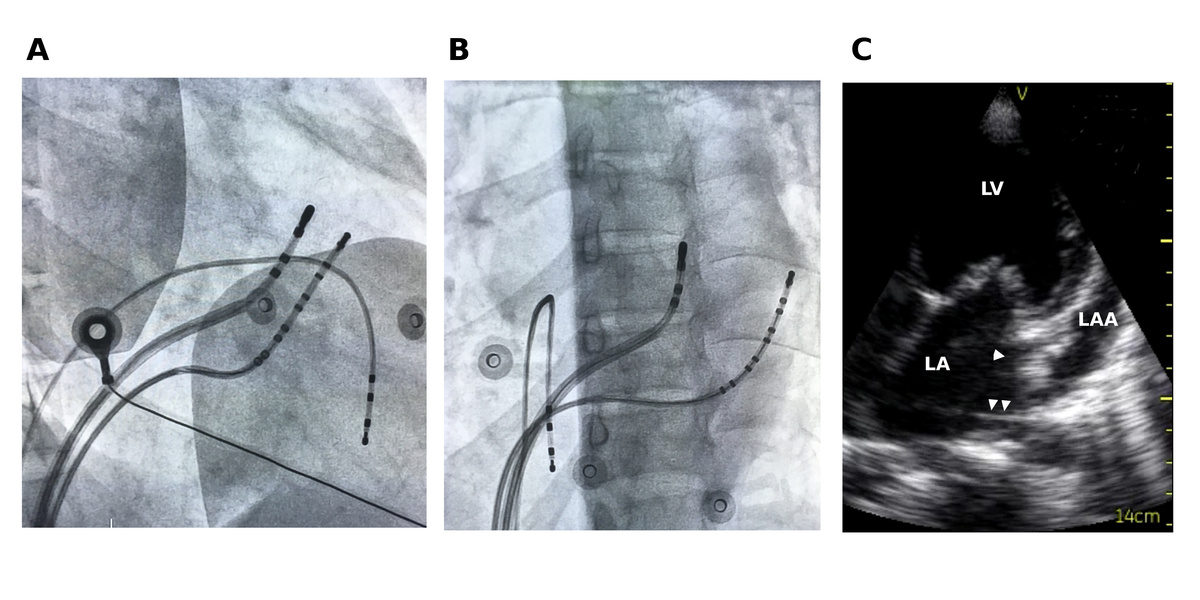
#5 Mapping in diverticulum - CSE potential most important
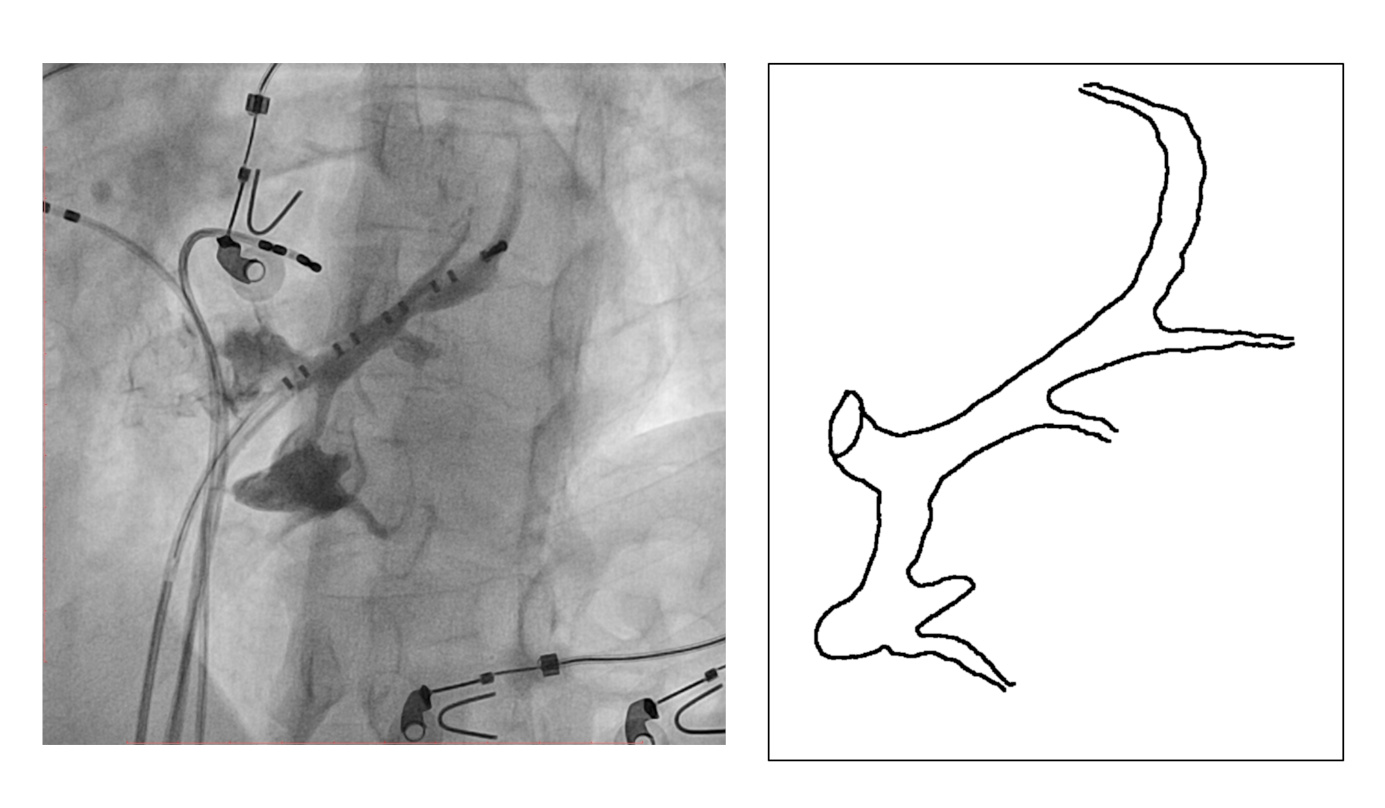
#5 Mapping in diverticulum - CSE potential most important
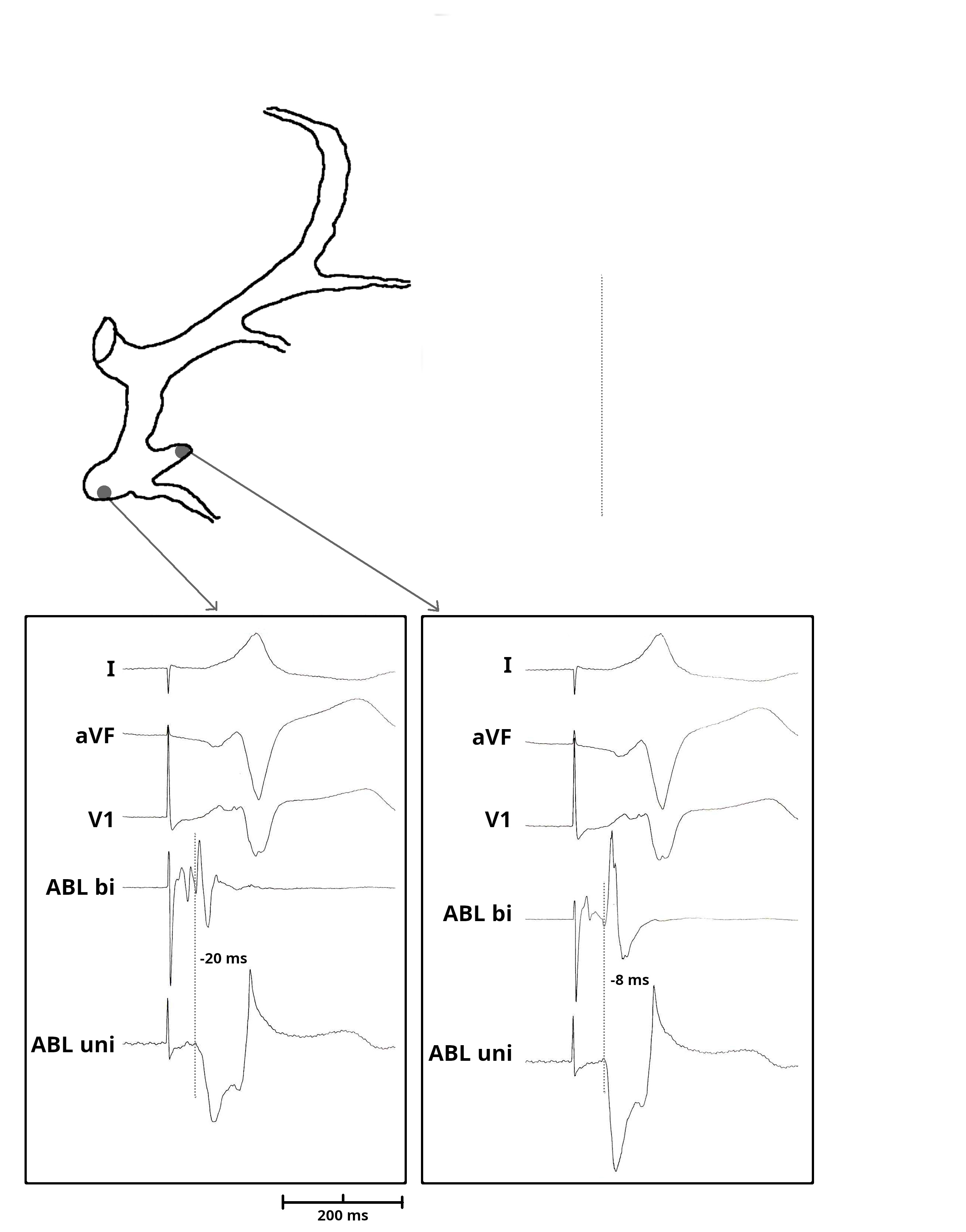
#5 Mapping in diverticulum - CSE potential most important
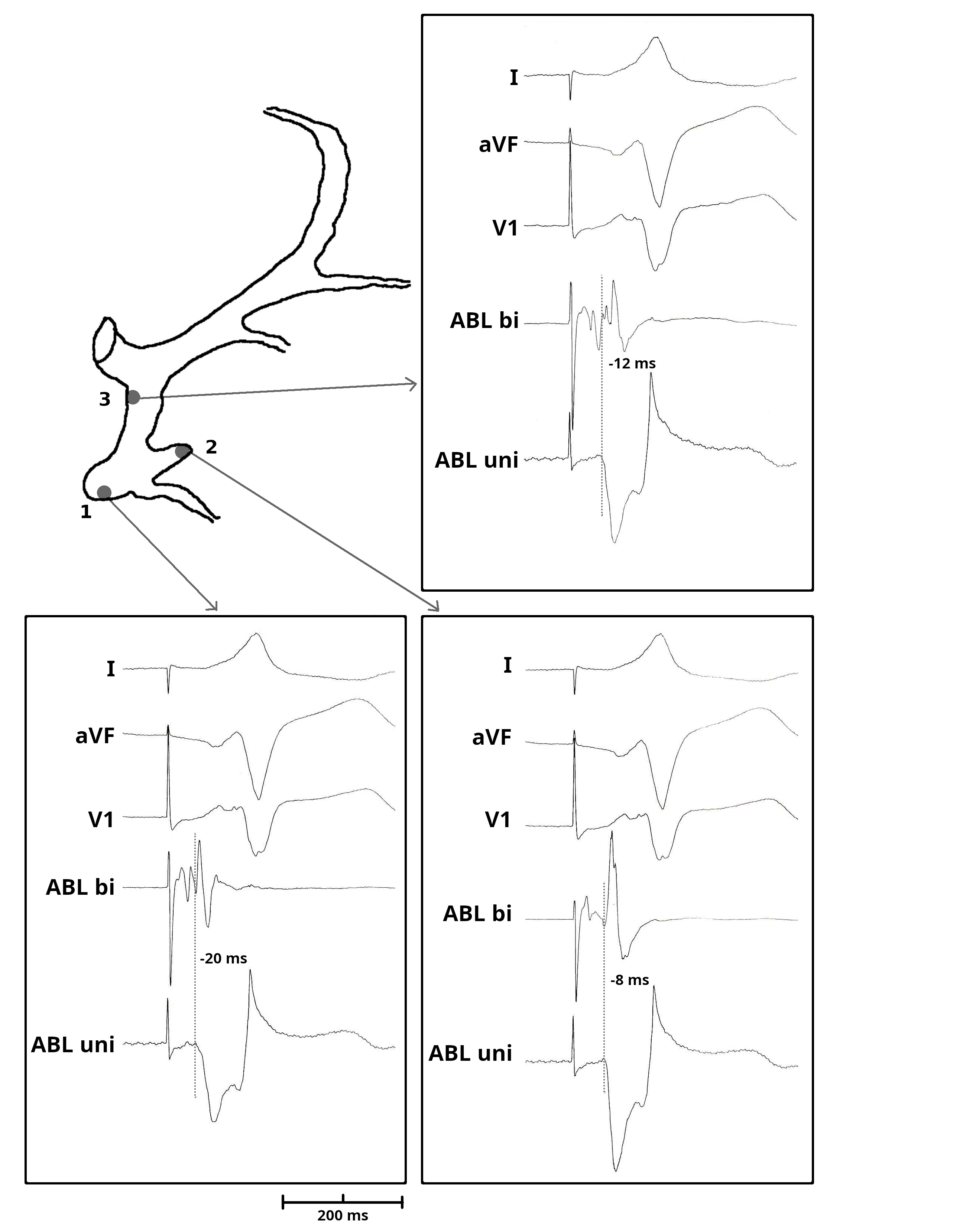
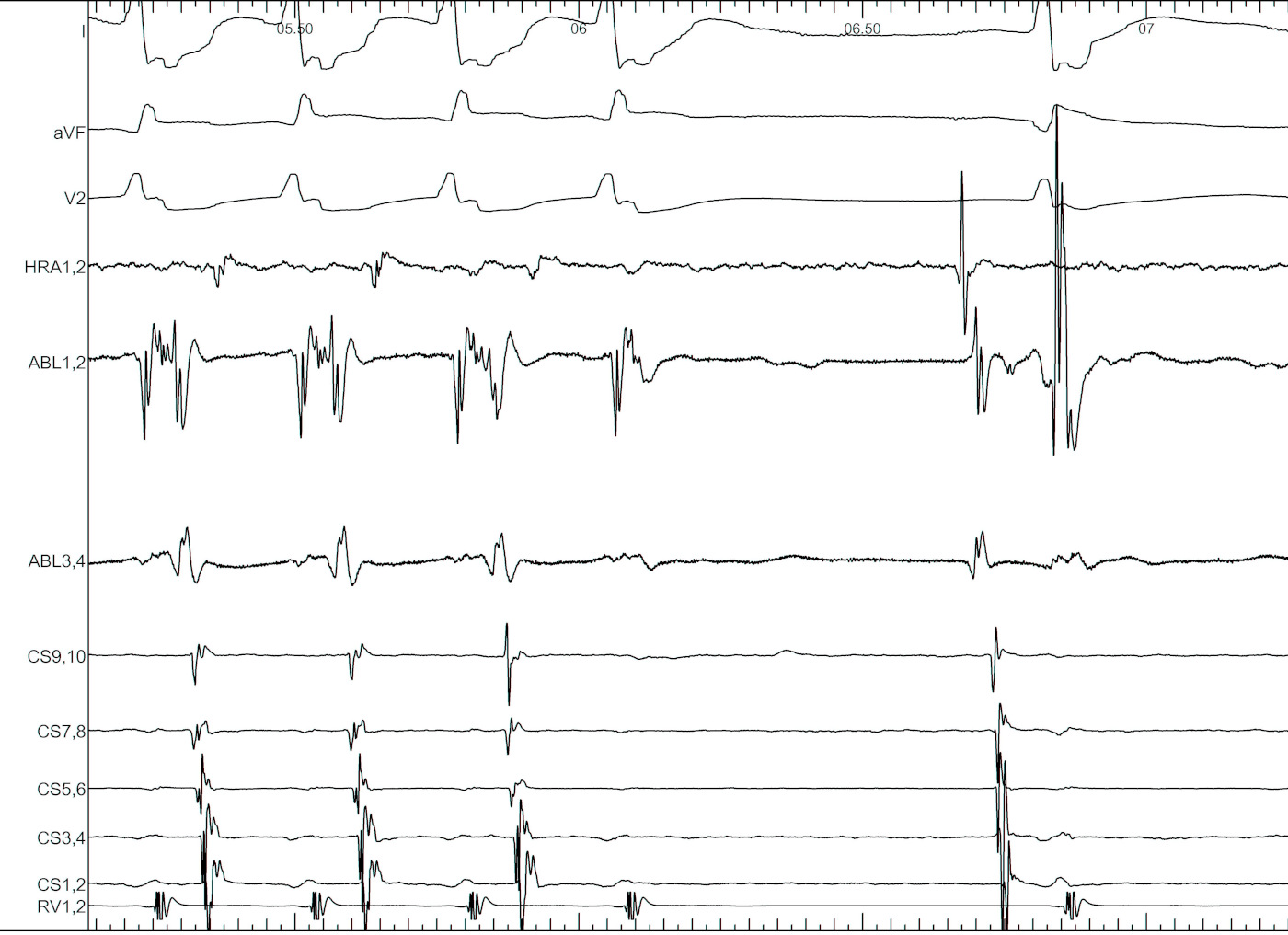
#6 Oblique pathways - Earliest A / V may be distant
#6 Oblique pathways - AP potential more important than earliest A
#7 Be afraid of ablating septal APs with A / V pacing
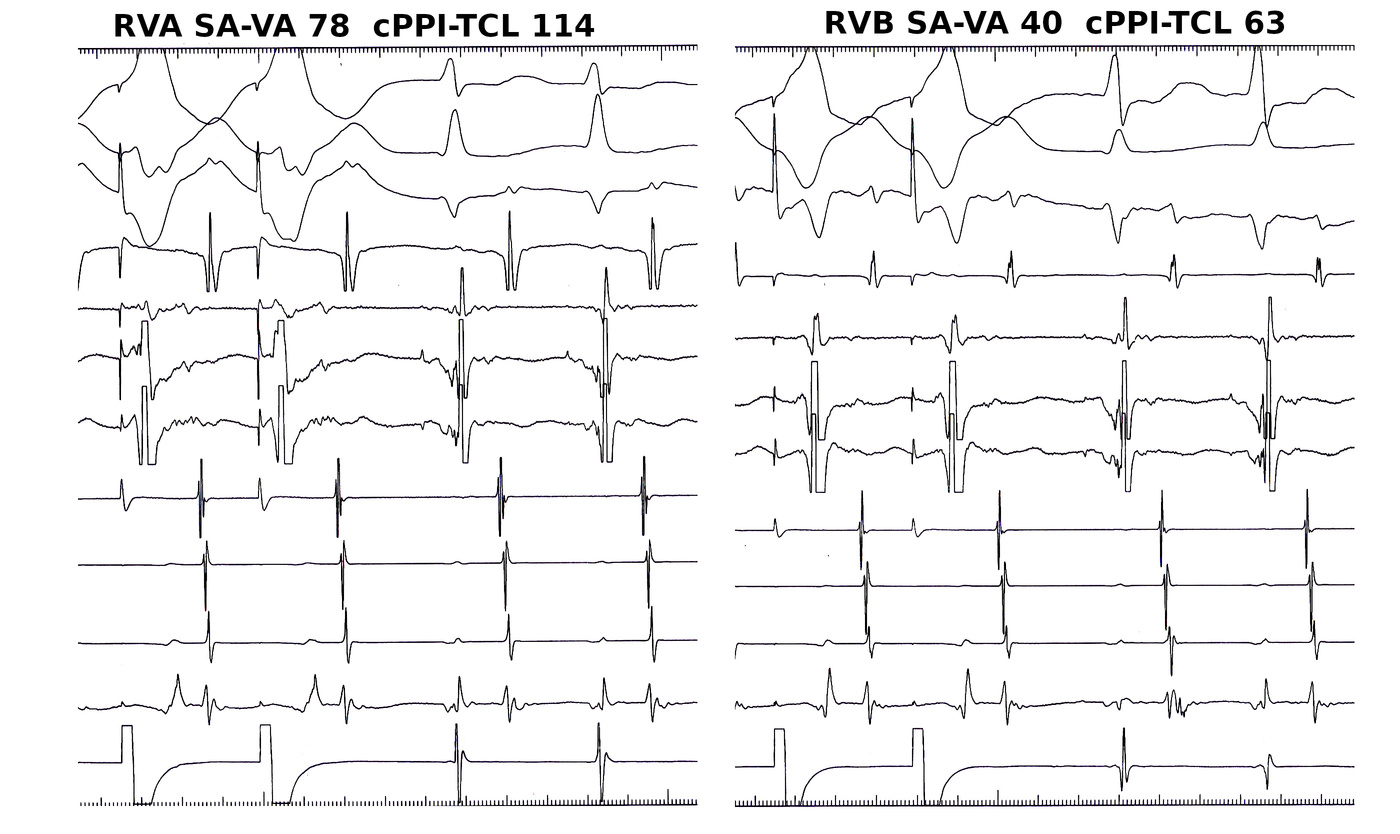
#8 When ablating in tachycardia, entrain the tachycardia

#9 Map anteroseptal AP from non coronary cusp
#10 Consider non annular location of AP
#10 Consider non annular location of AP
#11 Don't bump, but when it happens, use it

#12 Be aware of isthmus block