
Case 1
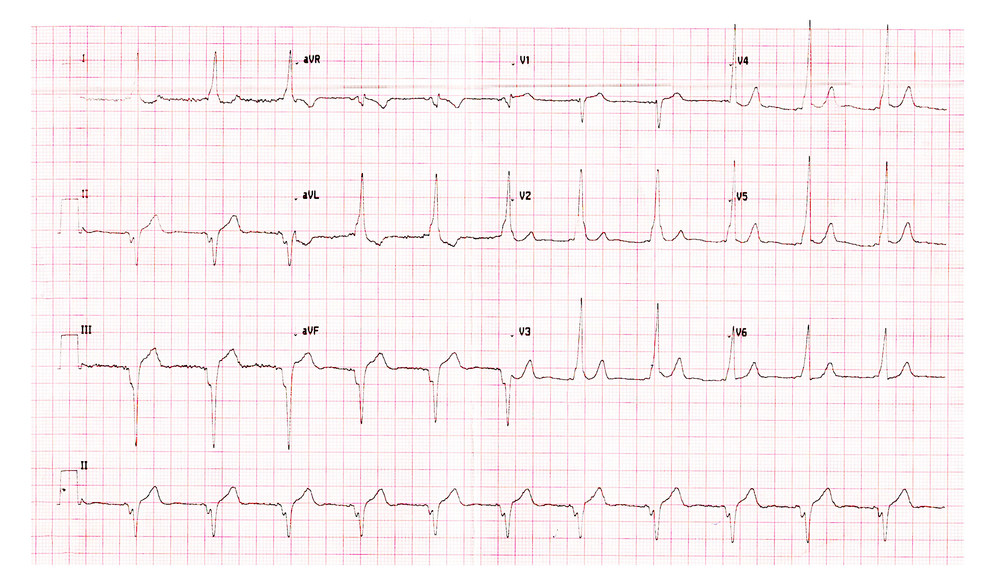
Male with palpitations
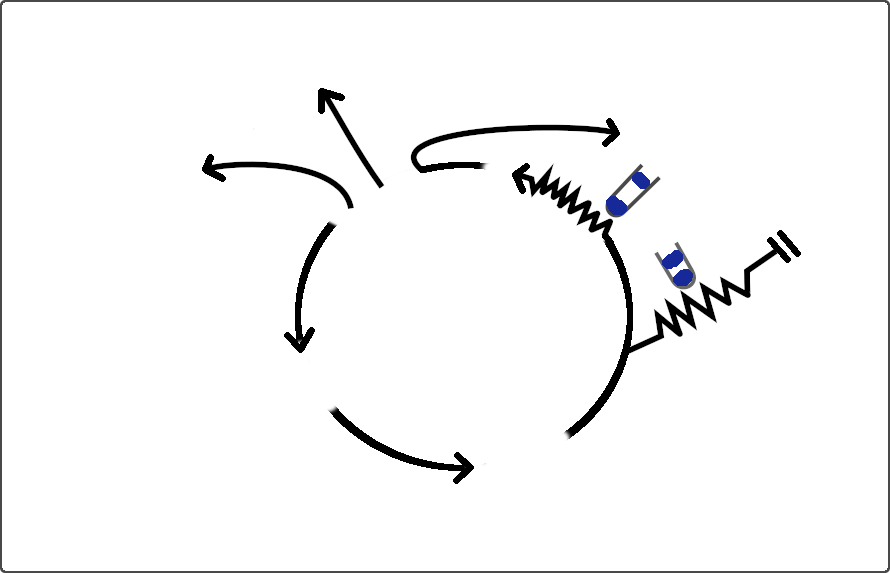
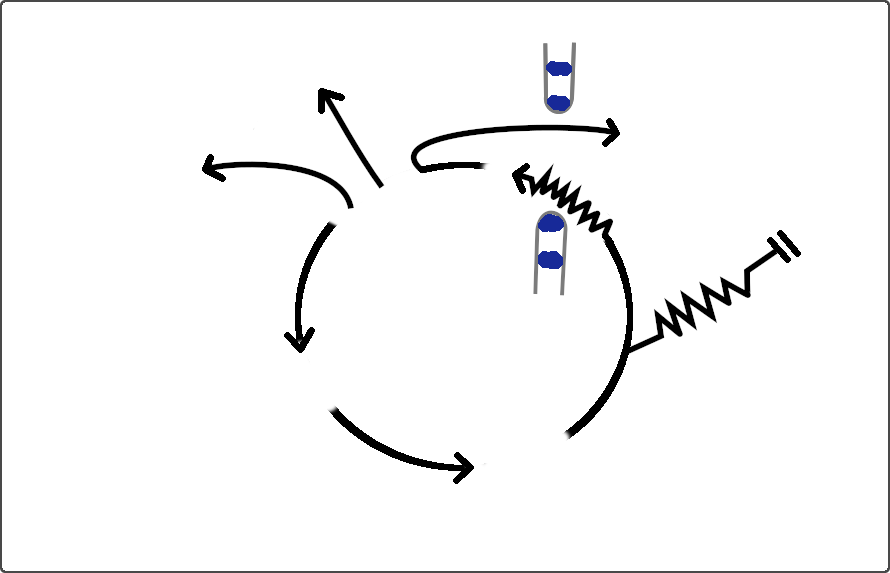
CS venogram
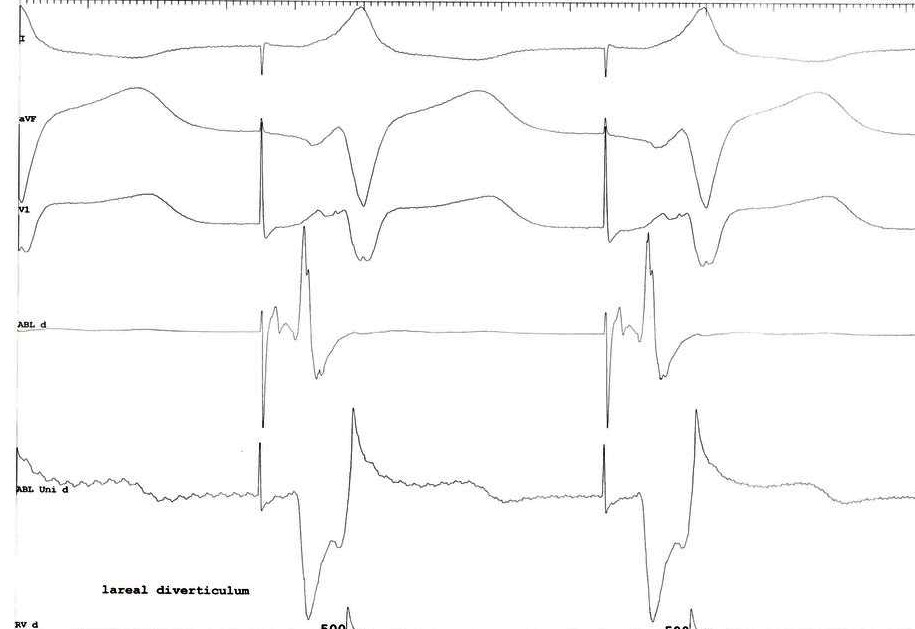
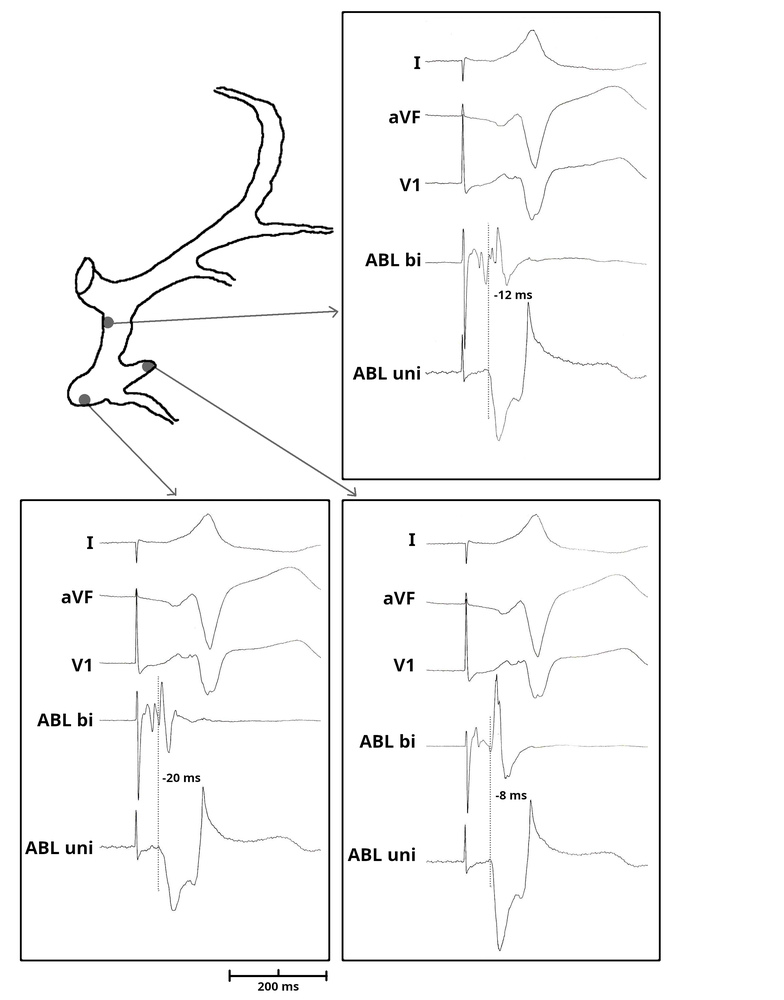
Mapping - lateral diverticulum
Mapping - medial diverticulum

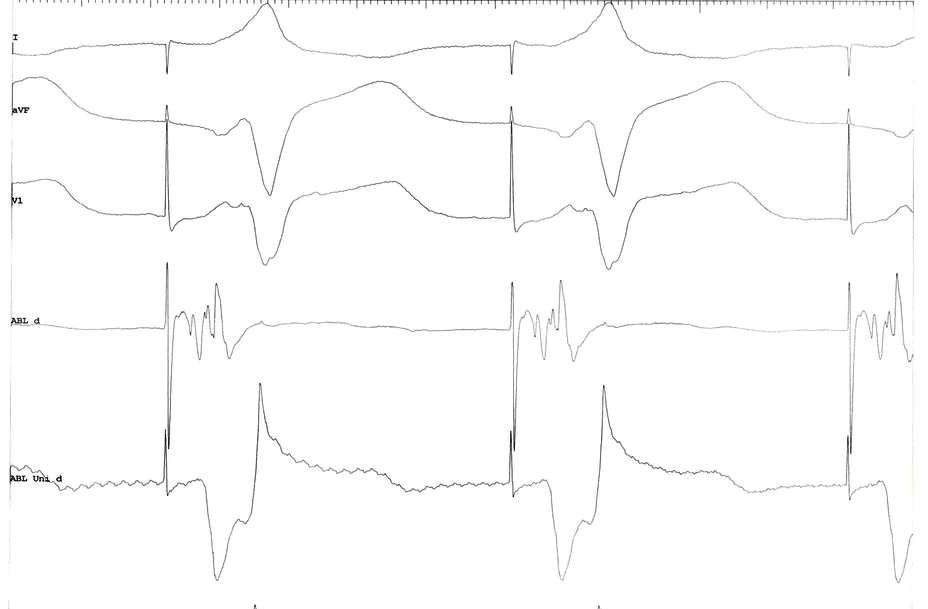
Mapping - neck
Mapping
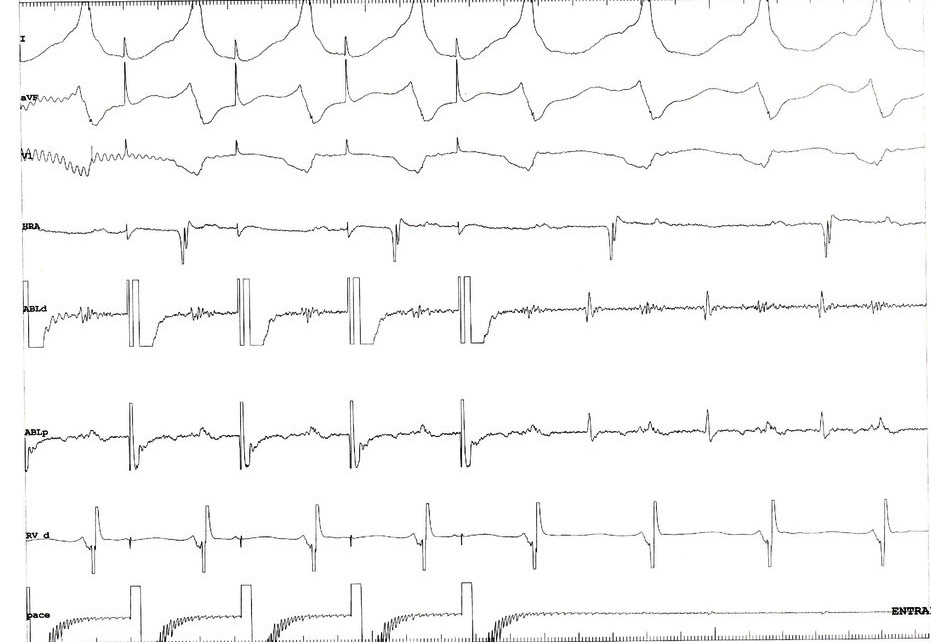
Mapping and ablation in CS diverticulum
Raja Selvaraj et al. J Interv Card Electrophysiol 2016 Nov 11;47(2):253-259.
Learning points
- Important to suspect diverticulum from ECG and look for it
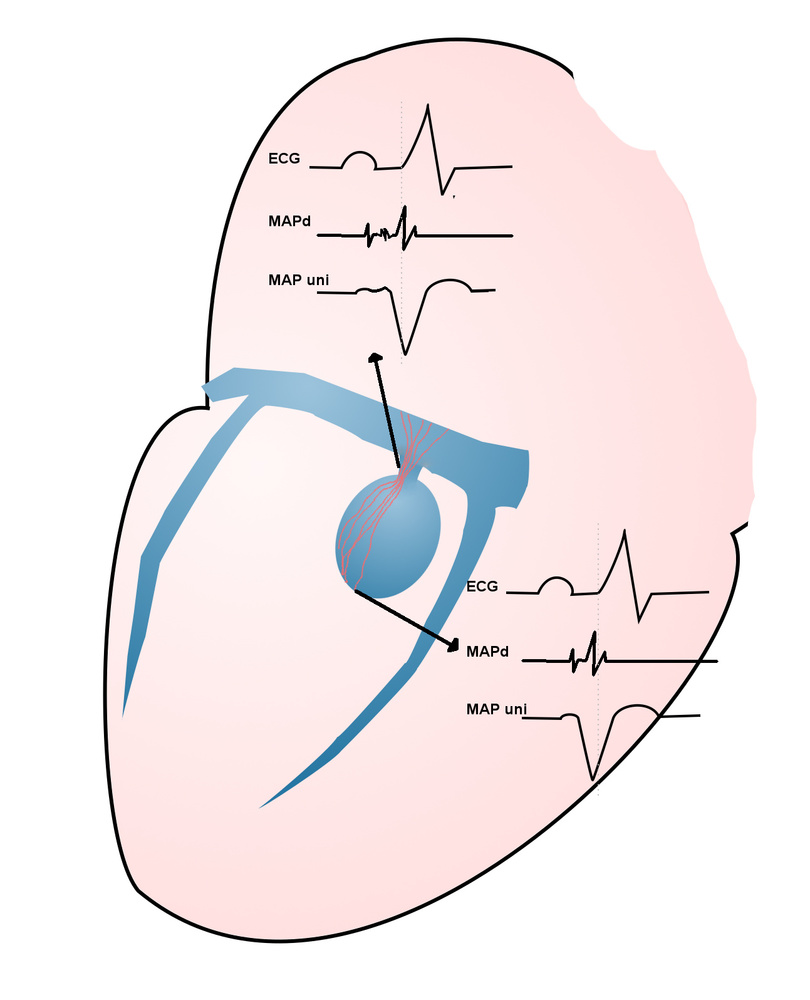
- Local V not as early as with AV pathways
- Mapping strategy more like atriofascicular - target body of pathway than the insertion
Case 2
Presentation
- 50 year old male
- Recurrent palpitations since last ten years
- Evaluation elsewhere 8 yrs back
- Mild LV dysfunction / RBBB / no documented tachycardia
- EP study - Inducible VT. Single chamber AICD implanted
- Referred now on noting ERI
Course
- On Amiodarone and beta blockers
- Occasional episodes, treated with ATP
- PG change done
- Presented with VT storm 3 months after PG change
Evaluation
- RBBB / LAD / normal PR on ECG
- Hypokinetic IVS and RV apex, LVEF 47%
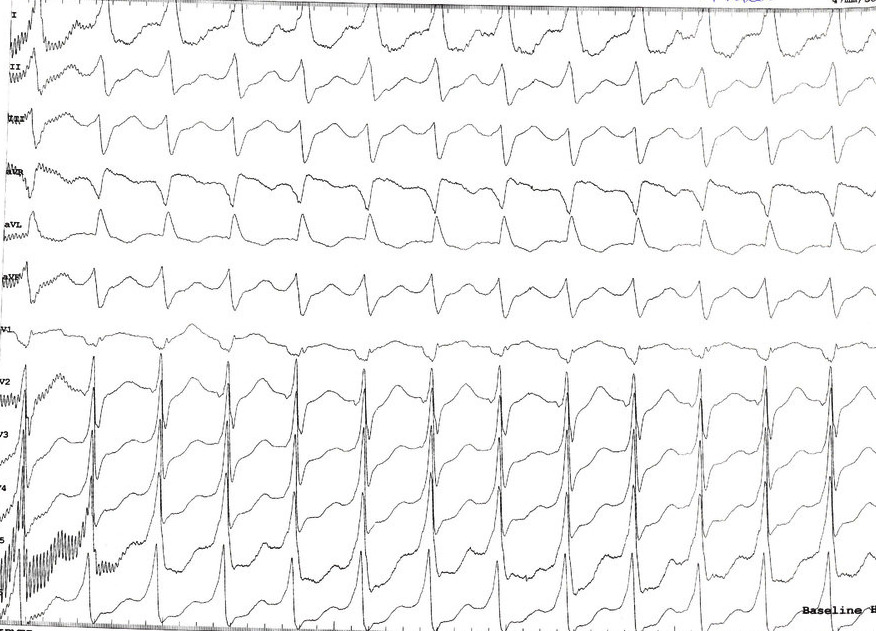
- ICD - Sustained tachycardia at ~ 300 - 350 ms, ATP mostly successful
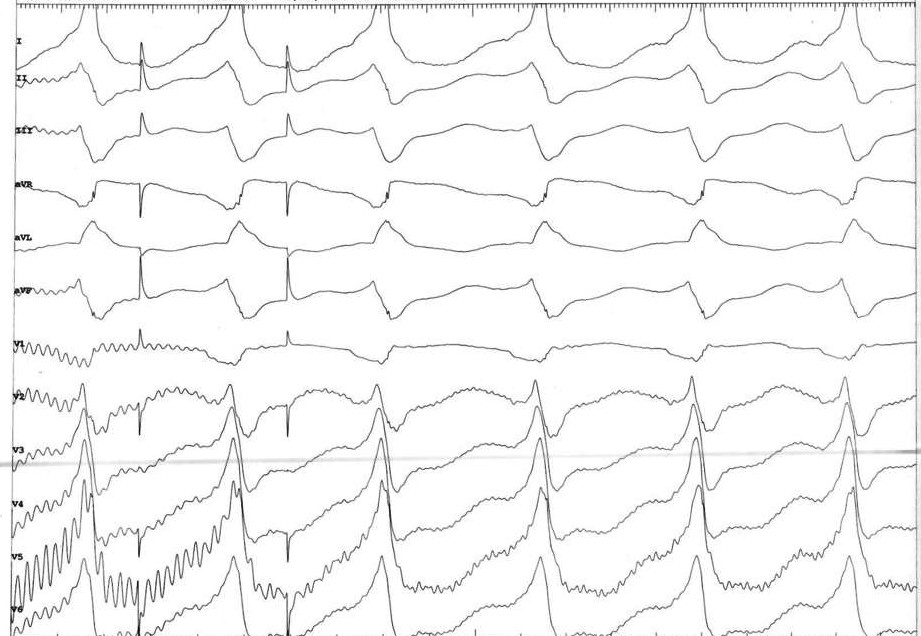
Regular WQRST in patient with RBBB / mild LV dysfunction
- SVT
- VT
- BBRT
EPS - Baseline
- RBBB, PR 150 ms
- HV 46 ms
- VAWB 540 ms
- AVWB 360 , AVERP 600/280
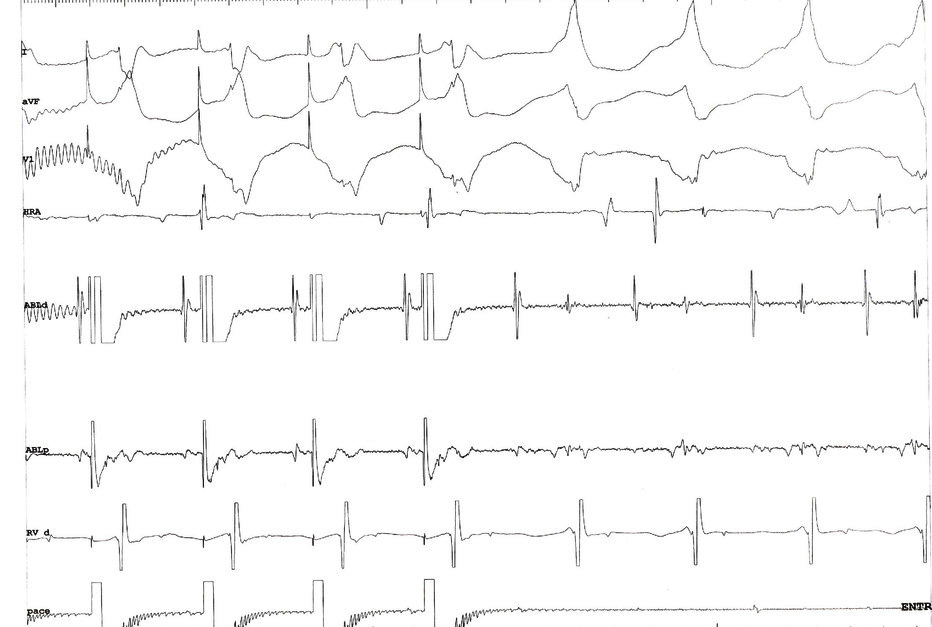
Tachycardia at beginning of case with VA dissociation - Mapping strategy ?
Mapping
- Started activation mapping in RV, but VT terminated
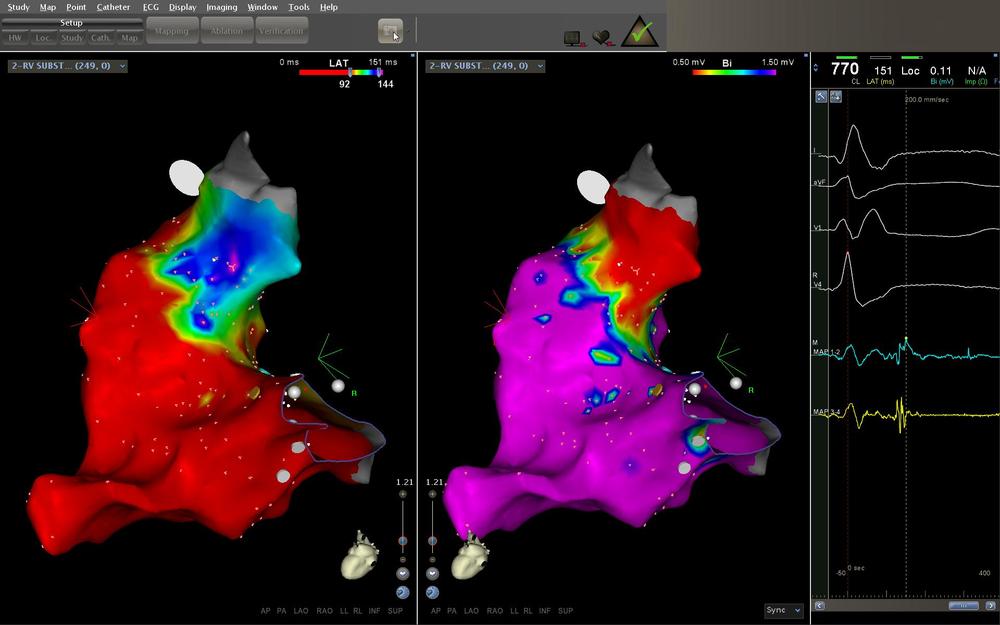
- Substrate mapping in RV
- Low voltage, late potentials and fractionated EGM in basal septum, low septal RVOT
RV substrate map - What next ?
Substrate based ablation
- Ablated at all regions with abnormal EGM
- Post ablation testing - VT inducible
- What next ?
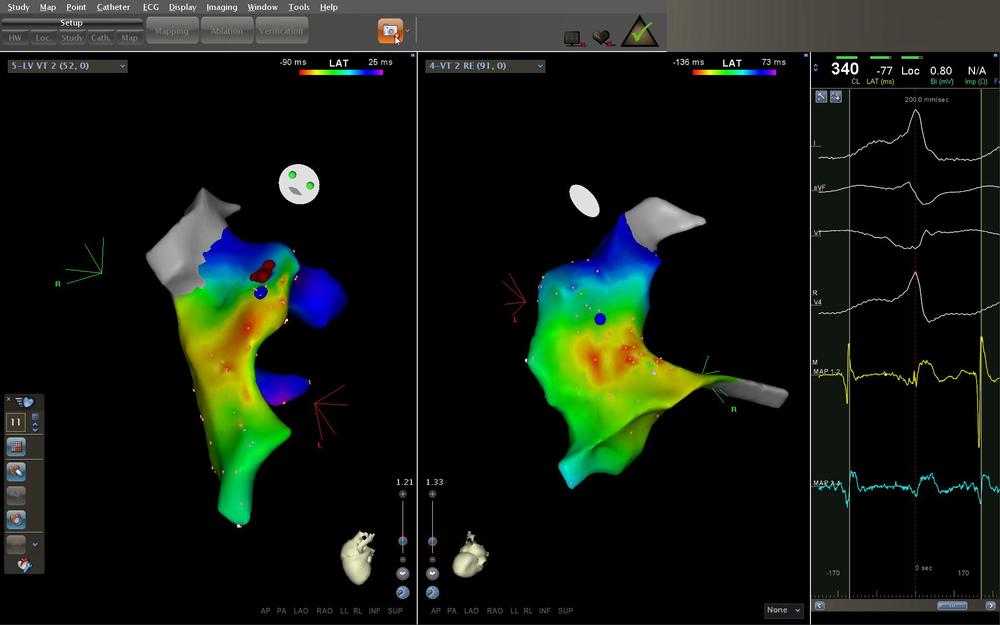
Activation map in RV - Double potentials on septum
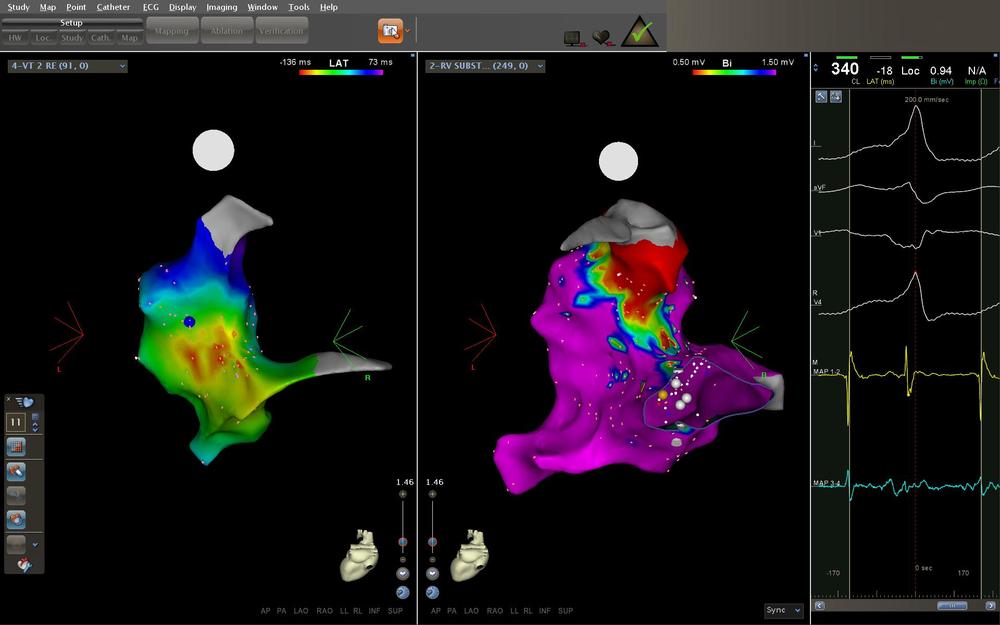
Diastolic potentials
Double potentials
Pacing from site
Interpretation
- Diatolic potential is far field
- Captured electrogram is systolic
- Manifest fusion
- PPI = TCL + ~ 35
- What do we do now ?
LV mapping - Double potentials on septum
Pacing from site
12 lead
Ablation

Learning points
- Double potentials - Pacing to identify local vs far-field
- Assimilate all info - PPI itself sometimes grey area
- Septal sites - always consider substrate on other side