
Case 1 - Accessory pathway ablation
- 47 year old male
- Recurrent palpitations with documented SVT
- Two failed previous ablations
Marks et al. JCE 2020. DOI: 10.1111/jce.14434
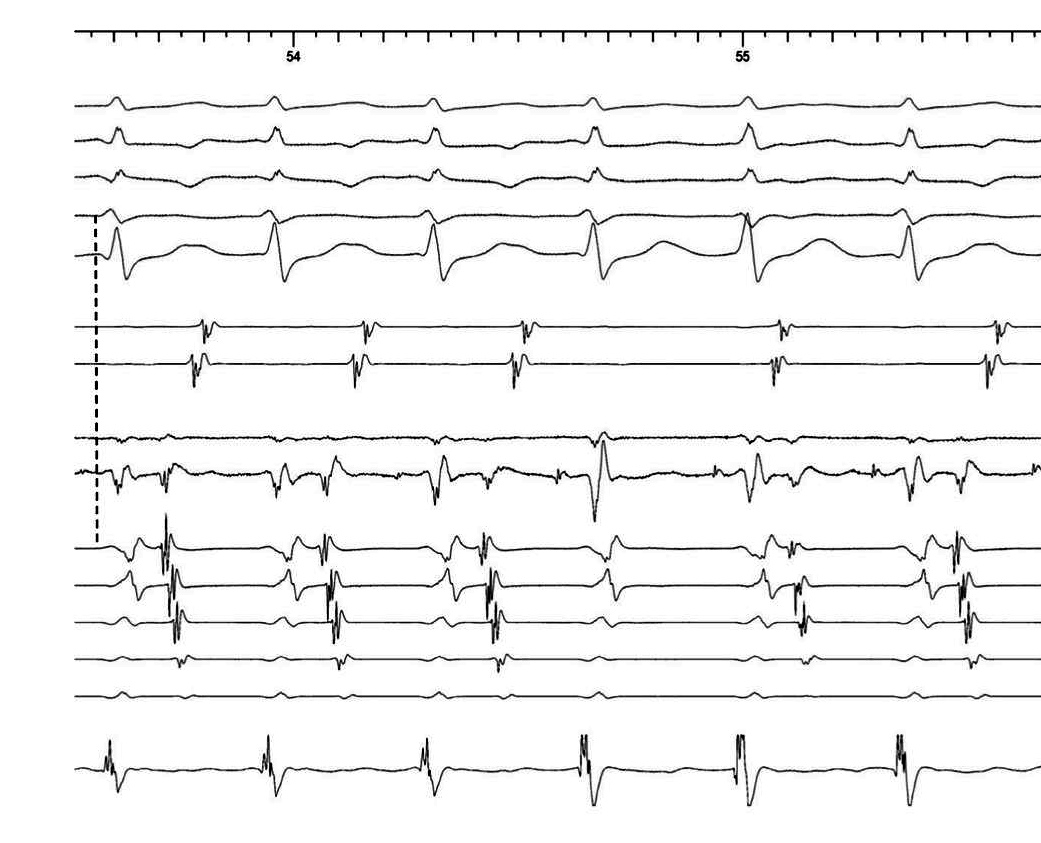
Sinus rhythm - Map catheter in anterior CS os
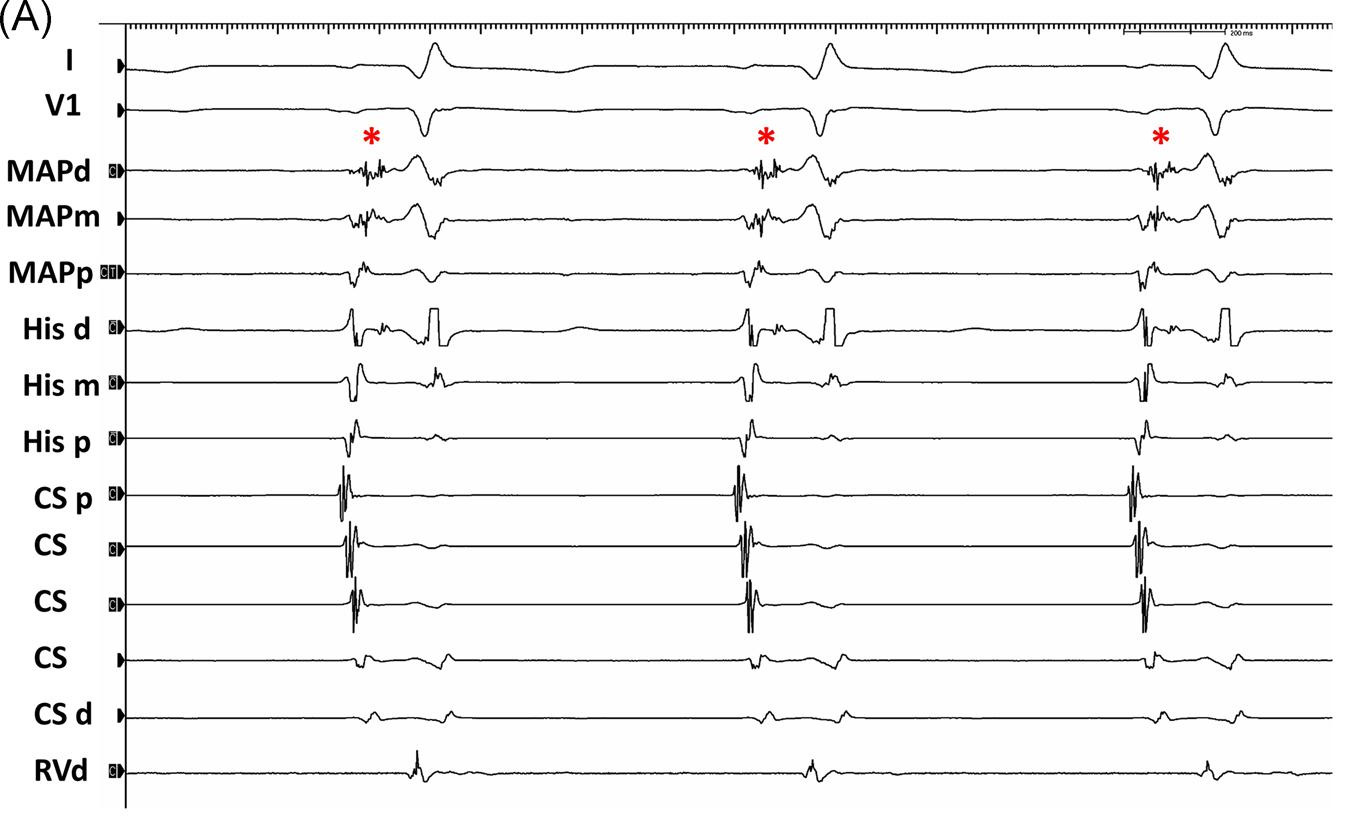
Fractionated signal
- Fractionated A from previous ablation
- AP potential
- His signal
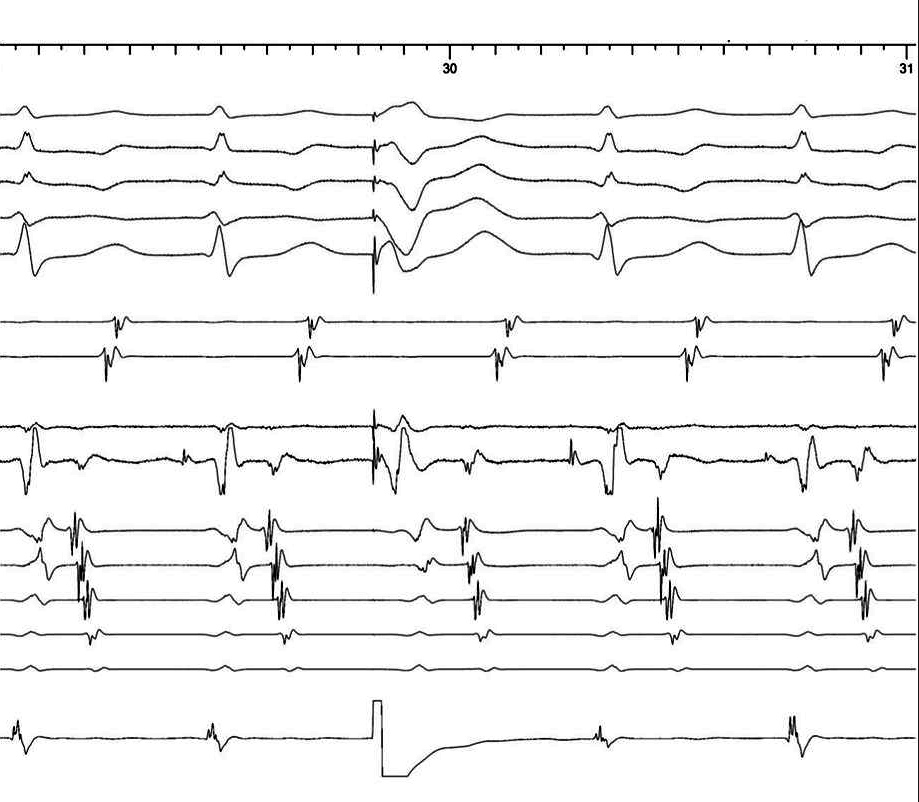
Tachycardia induction with burst atrial pacing
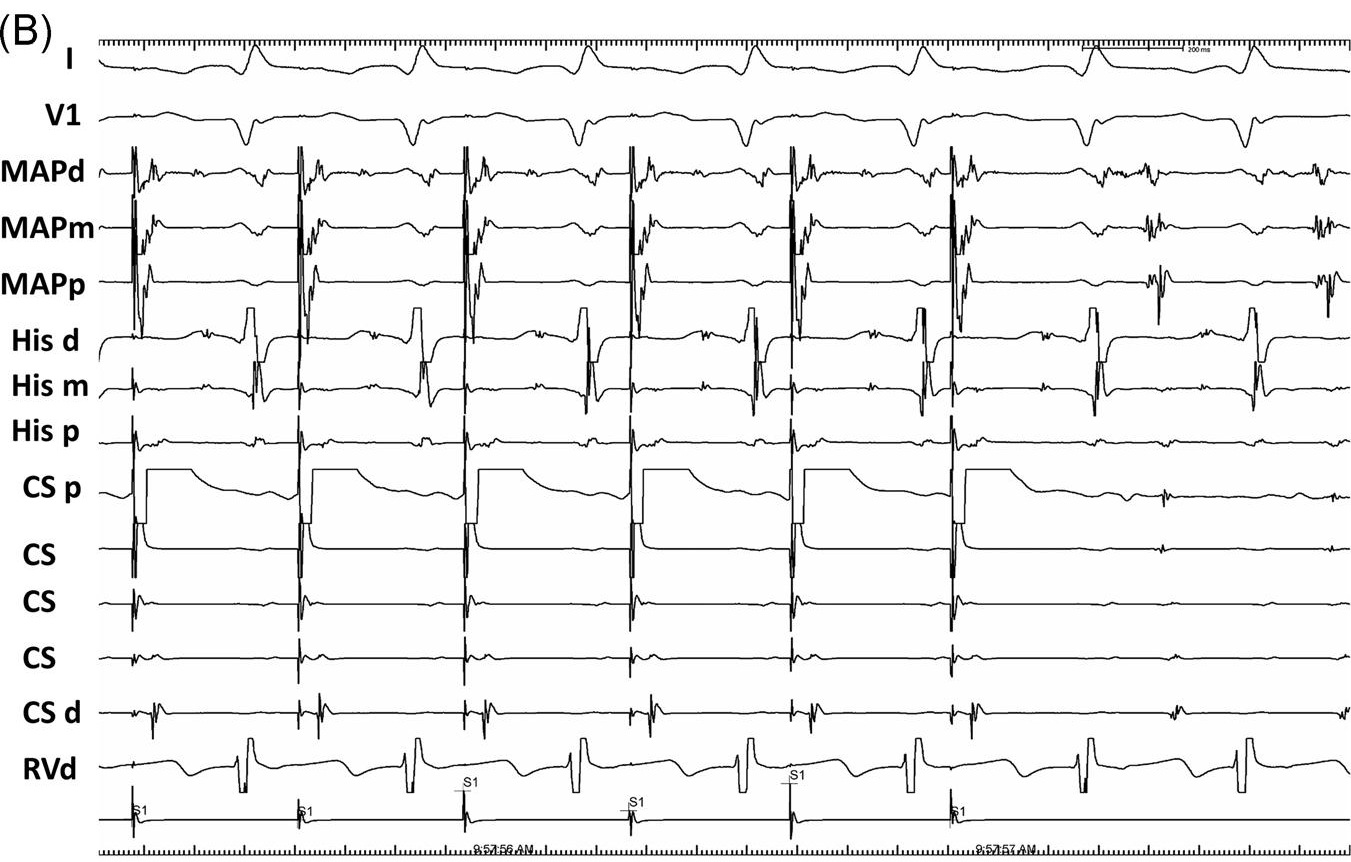
Findings
- Decremental conduction from A to signal
- Tachycardia induction associated with block to signal
- During tachycardia, signal seen after V
Mapping
- Earliest A during tachycardia - high, posterior CS os
- AP potential more anterior and inferior
- Where to ablate ?
Learning points
- Diagnostic catheter used for mapping
- Ablation at AP potential better than earliest A
- Difficult PSAP - consider epicardial AP, map within CS
Case 2 - Parahisian pacing
- 21 year old female
- Narrow QRS tachycardia
- Terminated with adenosine
Kara et al. JCE 2020. DOI: 10.1111/jce.14334
Parahisian pacing - What is the interpretation ?

What is the interpretation ?
Recap
- Transition from RV to RV+HB capture resulted in VA block
- Long-short HH cycle - HA block anticipated
- HA block = VA block. Indicates nodal conduction
Learning points
- Parahisian - complex to interpret, but provides wealth of information
- VA block associated with short HH cycle suggests nodal conduction
Case 3 - Narrow QRS tachycardia
- 76 year old woman
- No structural heart disease
- Narrow QRS tachycardia
Wakamatsu et al. JCE 2019. DOI: 10.1111/jce.14131
ECG - What is the differential diagnosis ?
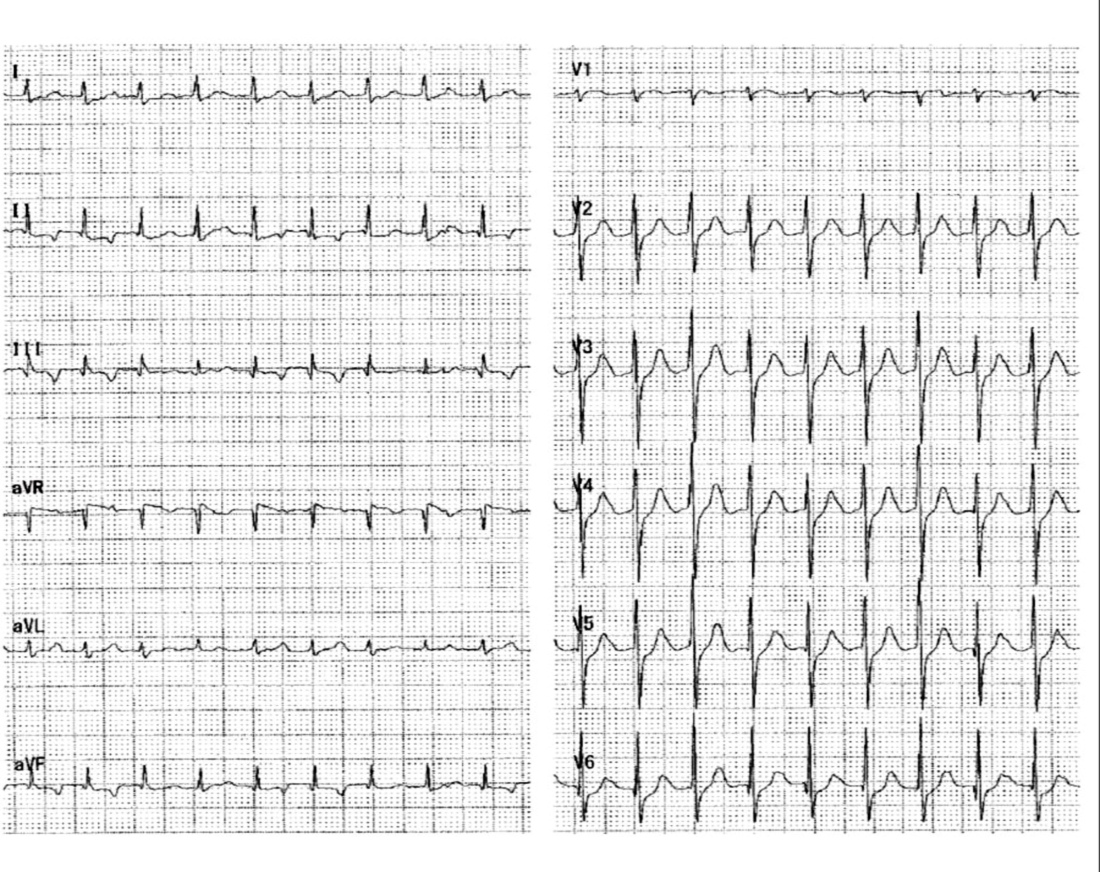
ECG
- Regular narrow QRS tachycardia
- 150 bpm
- V > A
- Possible 4:3 VA
- P waves inverted in inferior leads
Narrow QRS tachycardia with V > A
- Ventricular tachycardia
- AVNRT
- Junctional tachycardia
- Automatic
- Intra-His reentry
- Concealed nodoventricular AP with orthodromic AVRT
EP study
- CL / AH / HV - 634 / 90 / 46 ms
- RV pacing - earliest activation at prox CS, VAWB 480 ms
- RV extras - central, decremental
- Atrial extras - Two AH jumps - 320 ms and 290 ms
- Tachycardia induced by atrial burst pacing
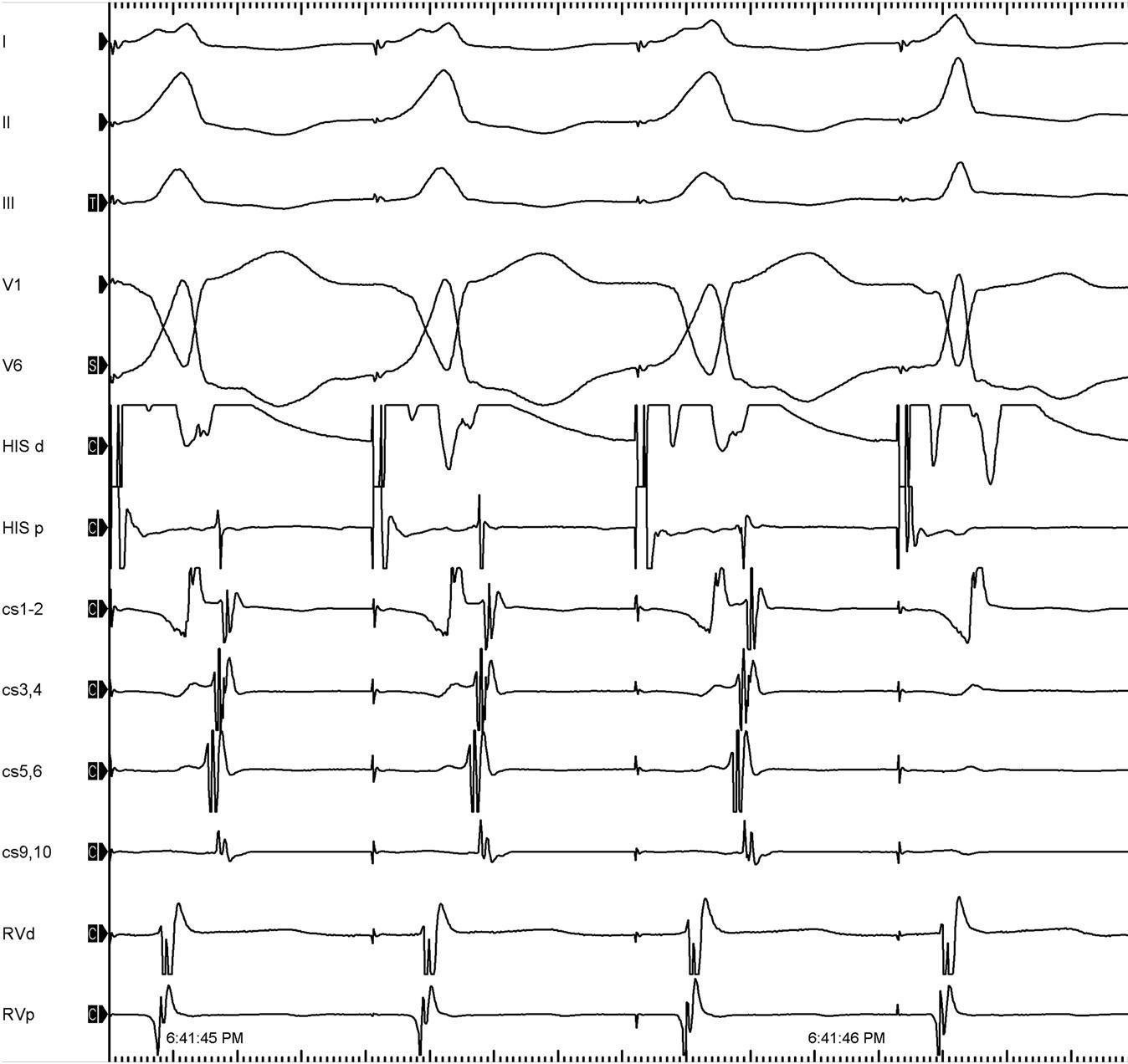
Intracardiac - Tachycardia
- Normal HV, not VT
- No split His - Not intra His reentry
- Change in A activation due to fusion with sinus
SVT with V > A, central A activation.
What now ?
- 1:1 conduction needed for pacing maneuvers
- Isoprenaline resulted in 1:1 VA
Ventricular extra during tachycardia
Ventricular overdrive pacing
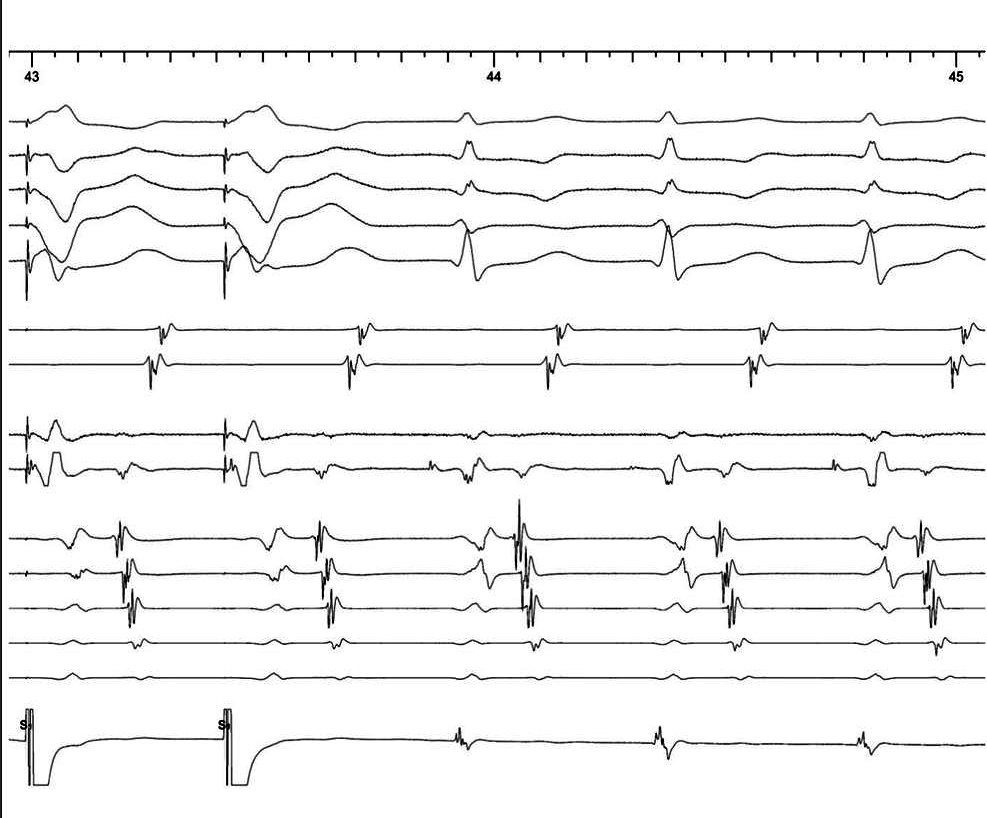
RV Pacing at 430 ms, 420 ms and during sinus
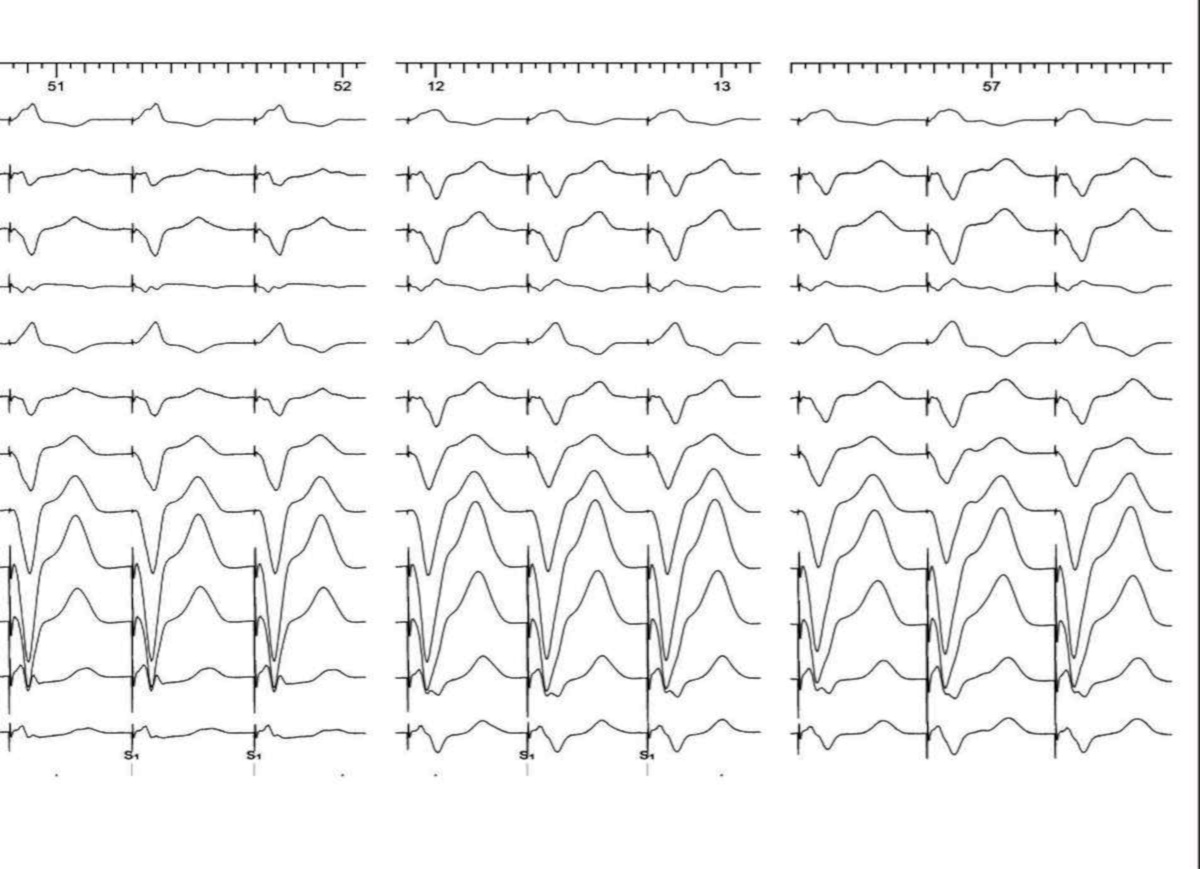
Recap
- His refractory PVC advances next His and advances subsequent A
- RVOP - VVA response (pseudo VAV), PPI-TCL 60 ms
- VA time longer than TCL
- Manifest fusion during entrainment from RV
- Diagnosis ?
Interpretation
- PPI-TCL and fusion consistent with ORT
- ORT with VA block - infranodal AP
- Fusion during entrainment - nodoventricular AP, not nodofascicular
- Very long VA time - bystander slow pathway
Schematic
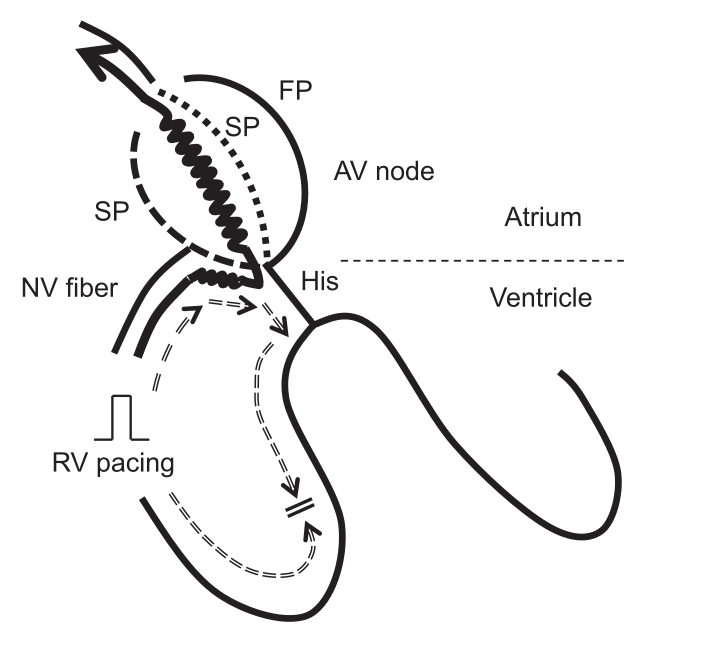
Management
- No discrete potential identified to ablate AP
- Anatomical slow pathway ablation done
- No further tachycardia
Learning points
- DD for NQRST with V > A
- Getting 1:1 VA with isoprenaline is critical
- Proper measurement with PVCs / RVOP is important
- Slow pathway ablation for NV AP - because of insertion into SP