
Introduction
Introduction
- CRT troubleshooting
- Not covering overlap with pacemaker troubleshooting
- Many aspects covered in previous talk
- In CRT, more than with other CIED, patient as whole more important
Outline of talk
- Non responders - Evaluation and management
- Deterioration after initial response
- Miscellaneous
CRT non responders
- Definition
- Potentially correctable causes
- Programming optimizations
- Other interventions
- Management in absence of correctable causes
CRT non responders
Definitions
- Clinical - Improvement in NYHA class
- Remodeling
- Reduction in LVESD / LVESV > 15%
- Increase in EF > 10 %
Prevalence
- Generally around one third
- Varies
- More if remodeling considered
Prevalence in our practice
- Super responders - 25%
- Responders - 30%
- Partial responders - 30%
- Non responders - 15%
Patient profile in major trials
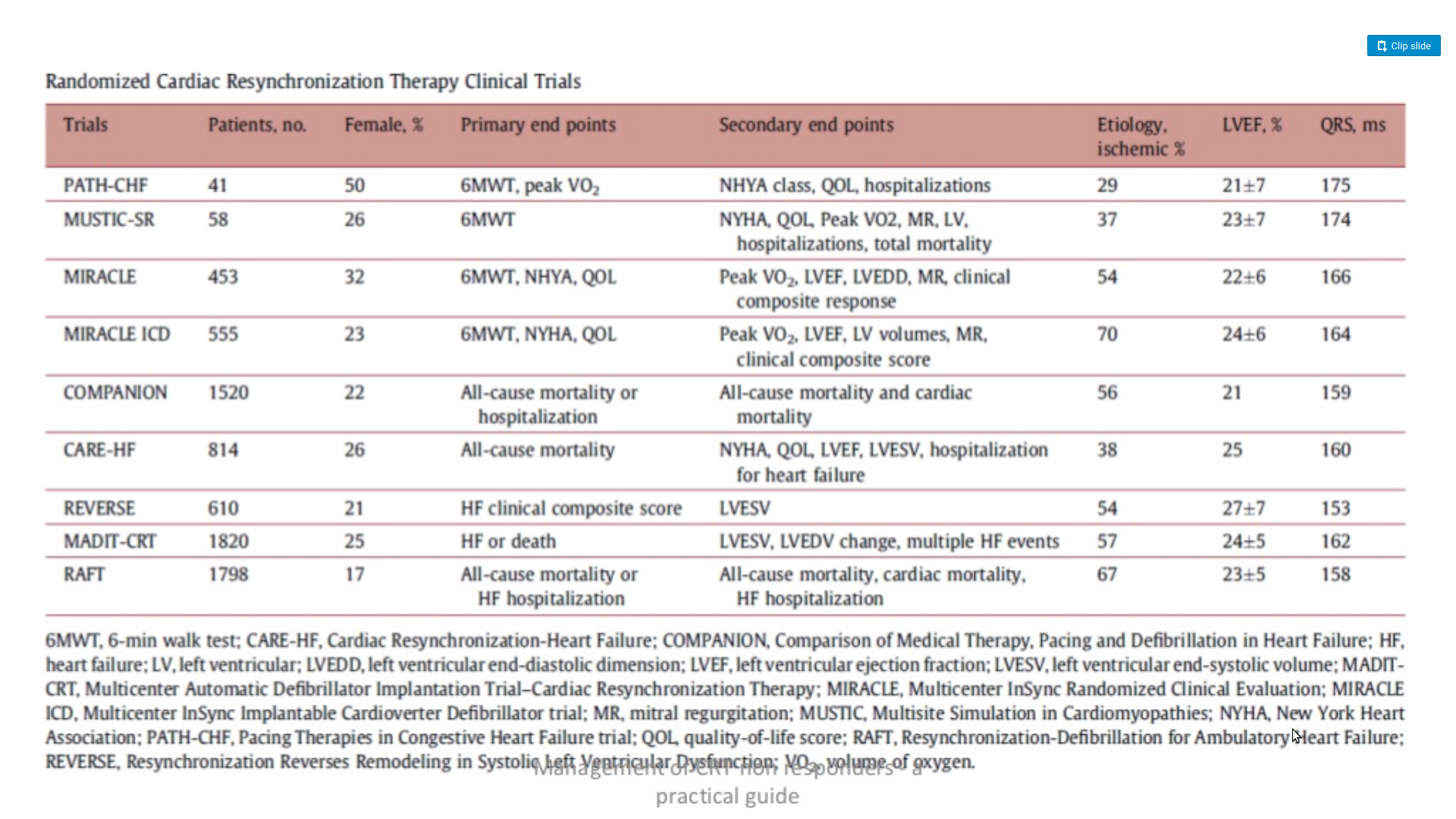
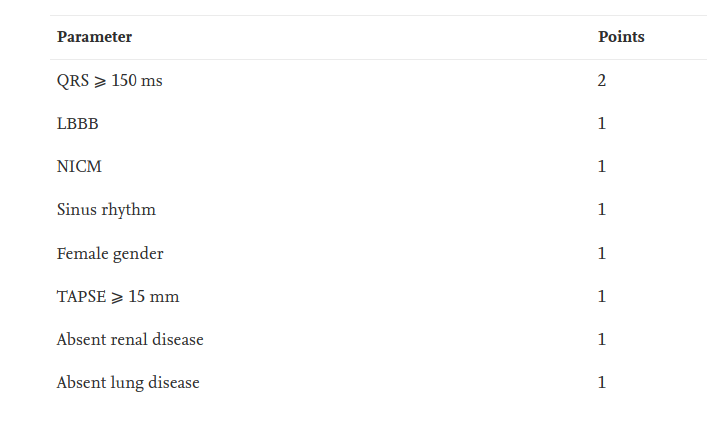
Patient selection matters
Mohamed Loutfi, Mostafa Nawar, Salah Eltahan, Aly Abo Elhoda, Predictors of response to cardiac resynchronization therapy in chronic heart failure patients, The Egyptian Heart Journal, Volume 68, Issue 4, 2016, Pages 227-236,
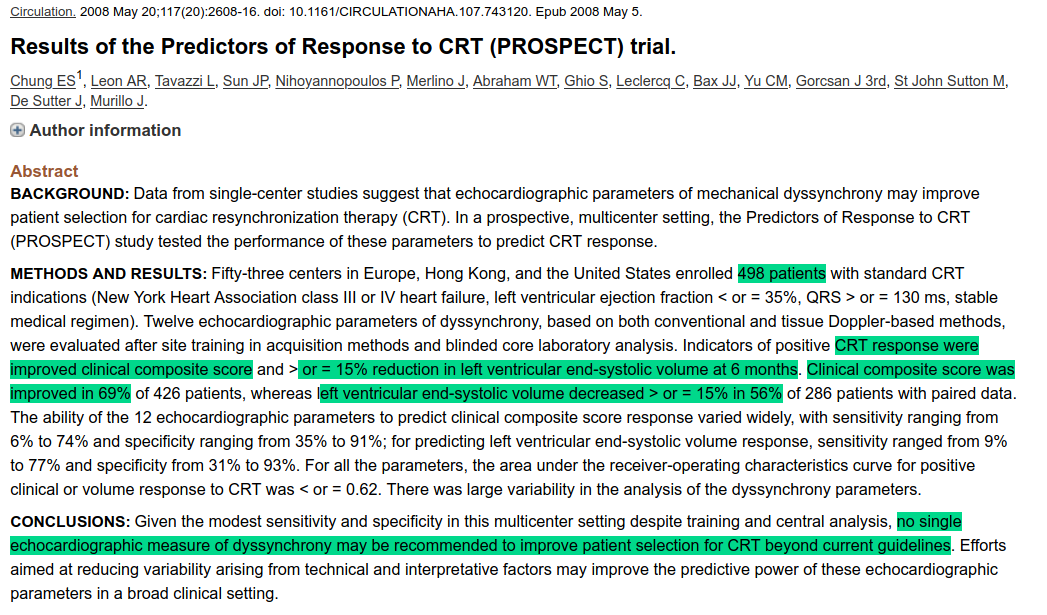
Echo not useful for selection
CRT follow up for response
- Evaluate at 3-6 months
- Complete normalization - Super responder
- Clinical and remodeling response - Responder
- Clinical or remodeling response - Partial responder
- No improvement - Non responder
Approach in non and partial responders
- Programmable reversible factors - Optimization
- Reversible factors not programmable - Lead revision
- No reversible factors
What to look for in device interrogation
- BiV paced percentage
- AV delay
- VV delay
- LV pacing polarity
BiV pacing percentage - At least 92%
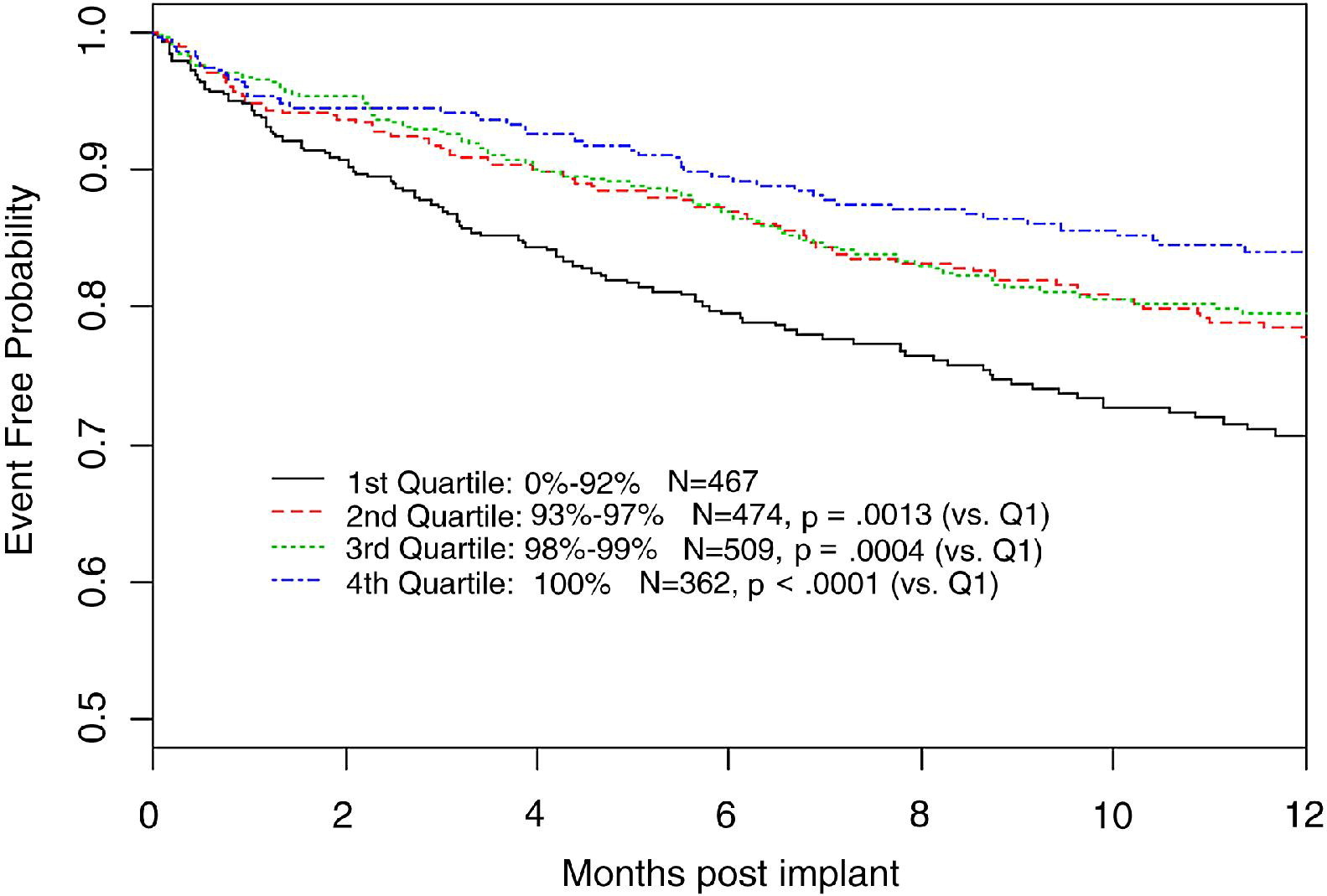
Koplan BA, Kaplan AJ, Weiner S, Jones PW, Seth M, Christman SA. Heart failure decompensation and all-cause mortality in relation to percent biventricular pacing in patients with heart failure: is a goal of 100% biventricular pacing necessary? J Am Coll Cardiol. 2009 Jan 27;53(4):355-60.
But preferably > 98% or AHARA
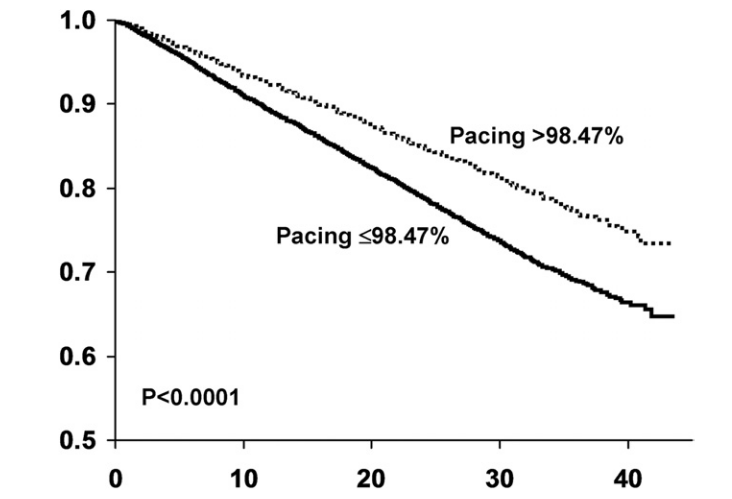
Hayes DL, Boehmer JP, Day JD, Gilliam FR 3rd, Heidenreich PA, Seth M, Jones PW, Saxon LA. Cardiac resynchronization therapy and the relationship of percent biventricular pacing to symptoms and survival. Heart Rhythm. 2011 Sep;8(9):1469-75
Causes of inadequate BiV pacing
- Rapid AV conduction (may be seen only with exercise !)
- Atrial arrhythmias, especially persistent AF
- Premature beats
Not all Vp are paced beats !
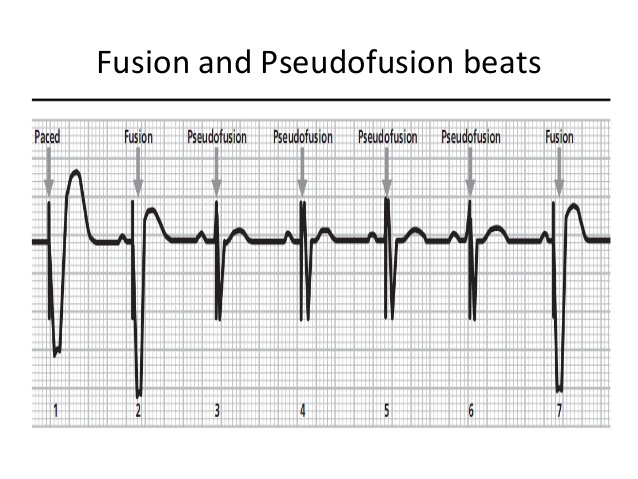
Inadequate BiV pacing despite high pacing percentage
- Irregularity with fusion beats
- Premature beats with fusion / pseudo fusion
- Long AV delay with fusion
- High LV threshold with intermittent / complete loss of capture
The problem of atrial fibrillation
- Patients with AF and >90% pacing in device records
- only 47% had >90% pacing when evaluated in Holter
Kamath GS, Cotiga D, Koneru JN, Arshad A, Pierce W, Aziz EF, Mandava A, Mittal S, Steinberg JS. The utility of 12-lead Holter monitoring in patients with permanent atrial fibrillation for the identification of nonresponders after cardiac resynchronization therapy. J Am Coll Cardiol. 2009 Mar 24;53(12):1050-5
Management of atrial fibrillation
- Good rate control
- Can still have suboptimal resynchronization due to irregularity
- Device algorithms may help
- Low threshold for AV node ablation
- Rhythm control - drugs / ablation
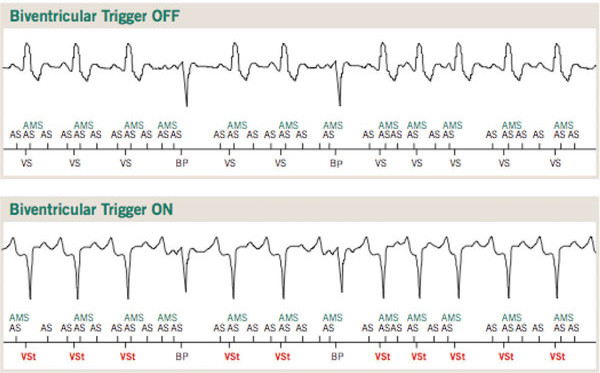
Device algorithms
- Ventricular sensed response / BiV trigger mode
- Atrial tracking recovery
- Conducted AF response
BiV trigger mode
AV nodal ablation
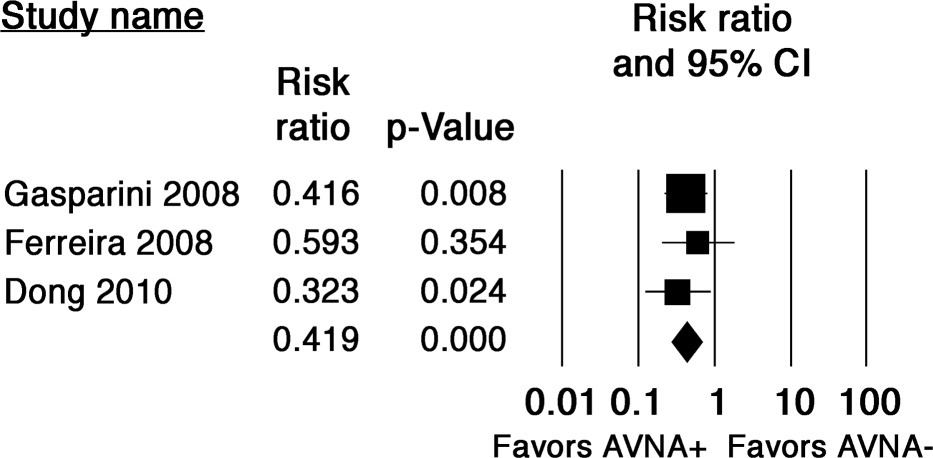
Ganesan AN, Brooks AG, Roberts-Thomson KC, Lau DH, Kalman JM, Sanders P. Role of AV nodal ablation in cardiac resynchronization in patients with coexistent atrial fibrillation and heart failure a systematic review. J Am Coll Cardiol. 2012 Feb 21;59(8):719-26
AV delay
Programming AV delay at implant
- Goal should be to pace with delay shorter than intrinsic AV conduction
- Initial value can be set based on PR interval
- Rate adaptive AV delay on
- AV delay optimization at implant not better than empiric AV delay (1)
- Ellenbogen KA, Gold MR, Meyer TE, Fernndez Lozano I, Mittal S, Waggoner AD, Lemke B, Singh JP, Spinale FG, Van Eyk JE, Whitehill J, Weiner S, Bedi M, Rapkin J, Stein KM. Primary results from the SmartDelay determined AV optimization: a comparison to other AV delay methods used in cardiac resynchronization therapy (SMART-AV) trial: a randomized trial comparing empirical, echocardiography-guided, and algorithmic atrioventricular delay programming in cardiac resynchronization therapy. Circulation. 2010 Dec 21;122(25):2660-8
AV delay optimization in non responders
- Echo guided - to optimize VTI / dp/dt
- MV inflow doppler - EA fusion / truncated A with diastolic MR / Ritters method
- ECG / exercise ECG to avoid fusion
Echo guided optimization
- Programming to AV delay based on best dp/dt
- Compared to empiric delay of 120 ms
- Better NYHA class and LVEF at 6 months
- Small study - 41 patients
Morales MA, Startari U, Panchetti L, Rossi A, Piacenti M. Atrioventricular delay optimization by doppler-derived left ventricular dP/dt improves 6-month outcome of resynchronized patients. Pacing Clin Electrophysiol. 2006 Jun;29(6):564-8
VV delay
VV delay optimization
- To achieve narrow QRS
- Echo guided
- ECG guided
- IEGM guided
QRS width and response
More narrowing of QRS associated with better response
Lecoq G, Leclercq C, Leray E, Crocq C, Alonso C, de Place C, Mabo P, Daubert C. Clinical and electrocardiographic predictors of a positive response to cardiac resynchronization therapy in advanced heart failure. Eur Heart J. 2005 Jun;26(11):1094-100
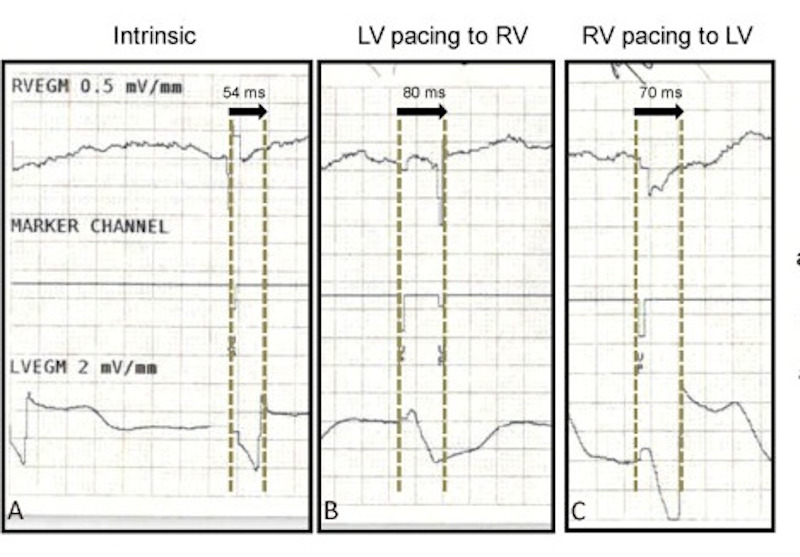
IEGM based method
0.5 ((R-LV - R-RV) + (IVCD-LR - IVCD-RL) )
Porciani MC, Rao CM, Mochi M, et al. A real-time three-dimensional echocardiographic validation of an intracardiac electrogram-based method for optimizing cardiac resynchronization therapy. Pacing Clin Electrophysiol. 2008;31:56–6
Surface ECG method
- time to sharp QRS onset with LV pacing (T1)
- time from RV pacing (T2)
- T1 - T2
Vidal B, Tamborero D, Mont L.. Brugada J. Electrocardiographic optimization of interventricular delay in cardiac resynchronization therapy:a simple method to optimize the device. J Cardiovasc Electrophysiol. 2007;18:1252–1257
Surface ECG method - by QRS width
Surface ECG - T1 T2 method
Automatic algorithms
- QuickOpt (St Jude)
- Smart AV (Bos)
- SonR (Sorin) - Accelerometer in RA lead
- Adaptive CRT (Medtronic)
Role of device algorithms for optimization
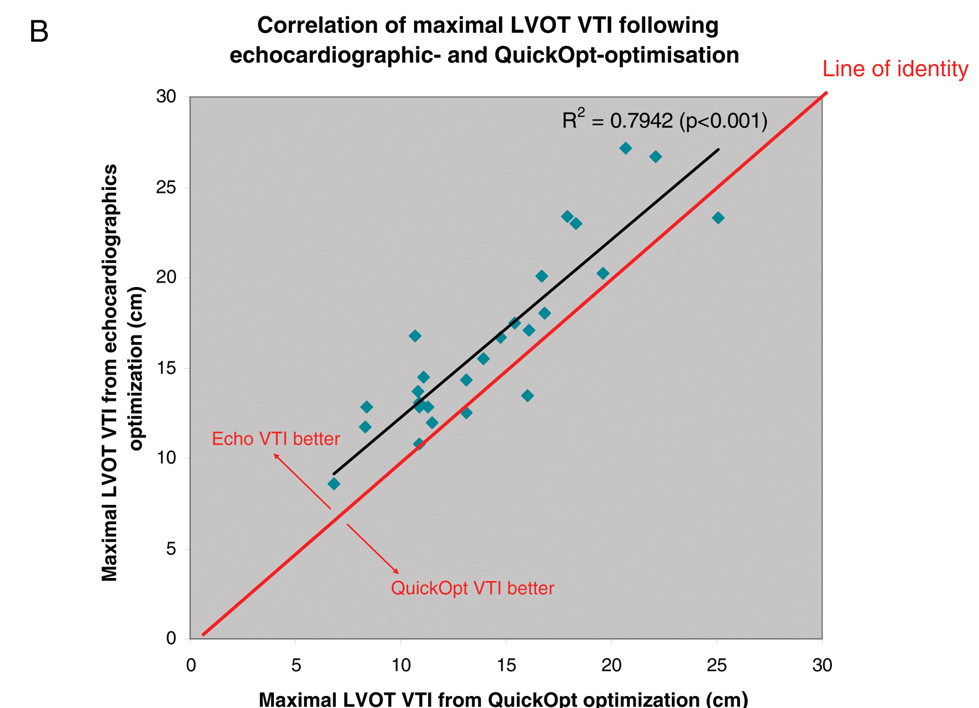
Kamdar R, Frain E, Warburton F, Richmond L, Mullan V, Berriman T, Thomas G, Tenkorang J, Dhinoja M, Earley M, Sporton S, Schilling R. A prospective comparison of echocardiography and device algorithms for atrioventricular and interventricular interval optimization in cardiac resynchronization therapy. Europace. 2010 Jan;12(1):84-91
Non programmable correction - Lead position
q-LV for selecting and assessing position
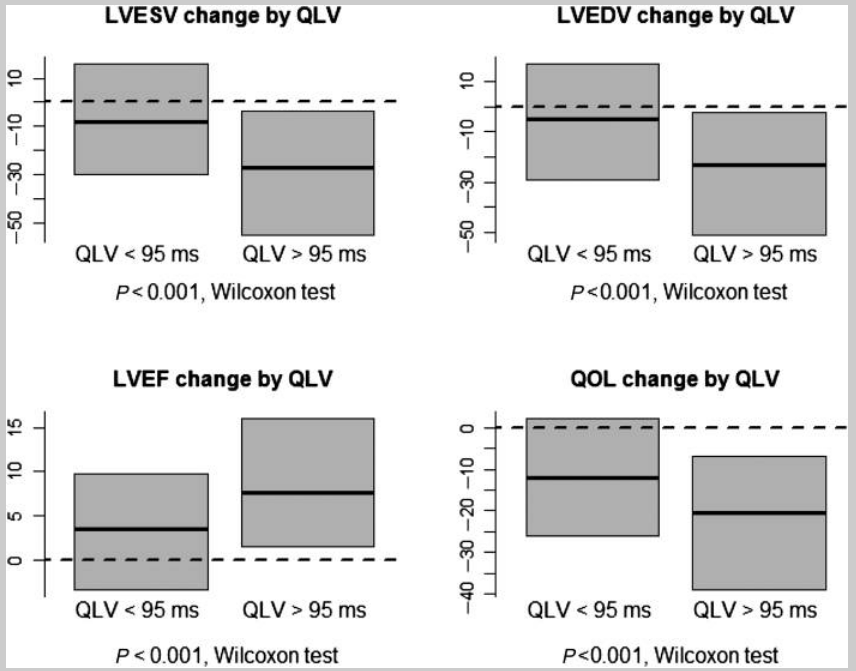
Gold MR, Birgersdotter-Green U, Singh JP, Ellenbogen KA, Yu Y, Meyer TE, Seth M, Tchou PJ. The relationship between ventricular electrical delay and left ventricular remodelling with cardiac resynchronization therapy. Eur Heart J. 2011 Oct;32(20):2516-24
RV lead position - no value in general
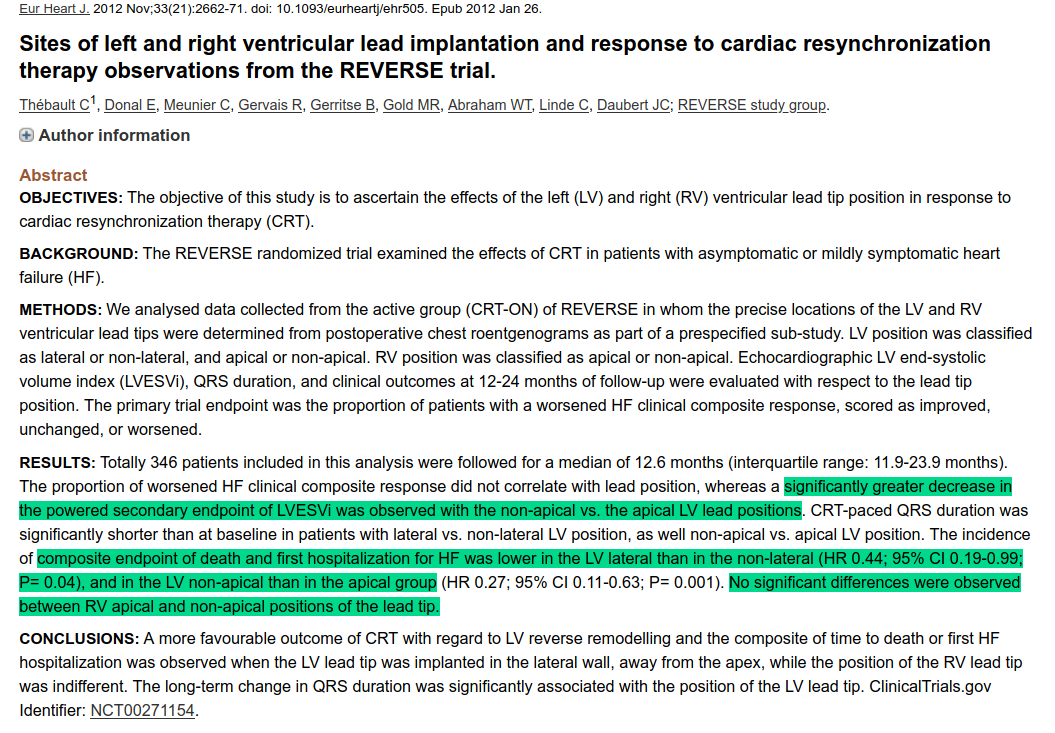
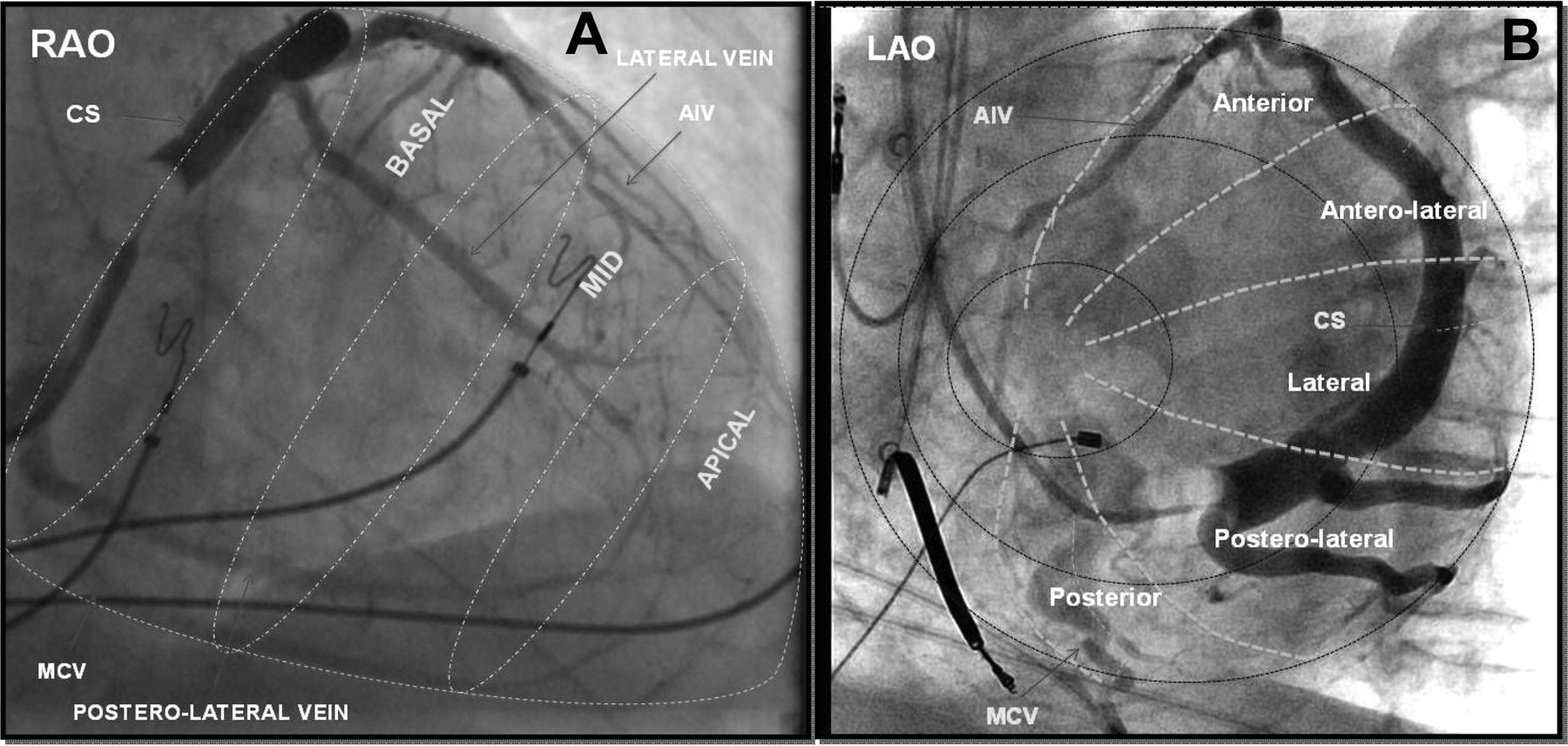
LV lead position
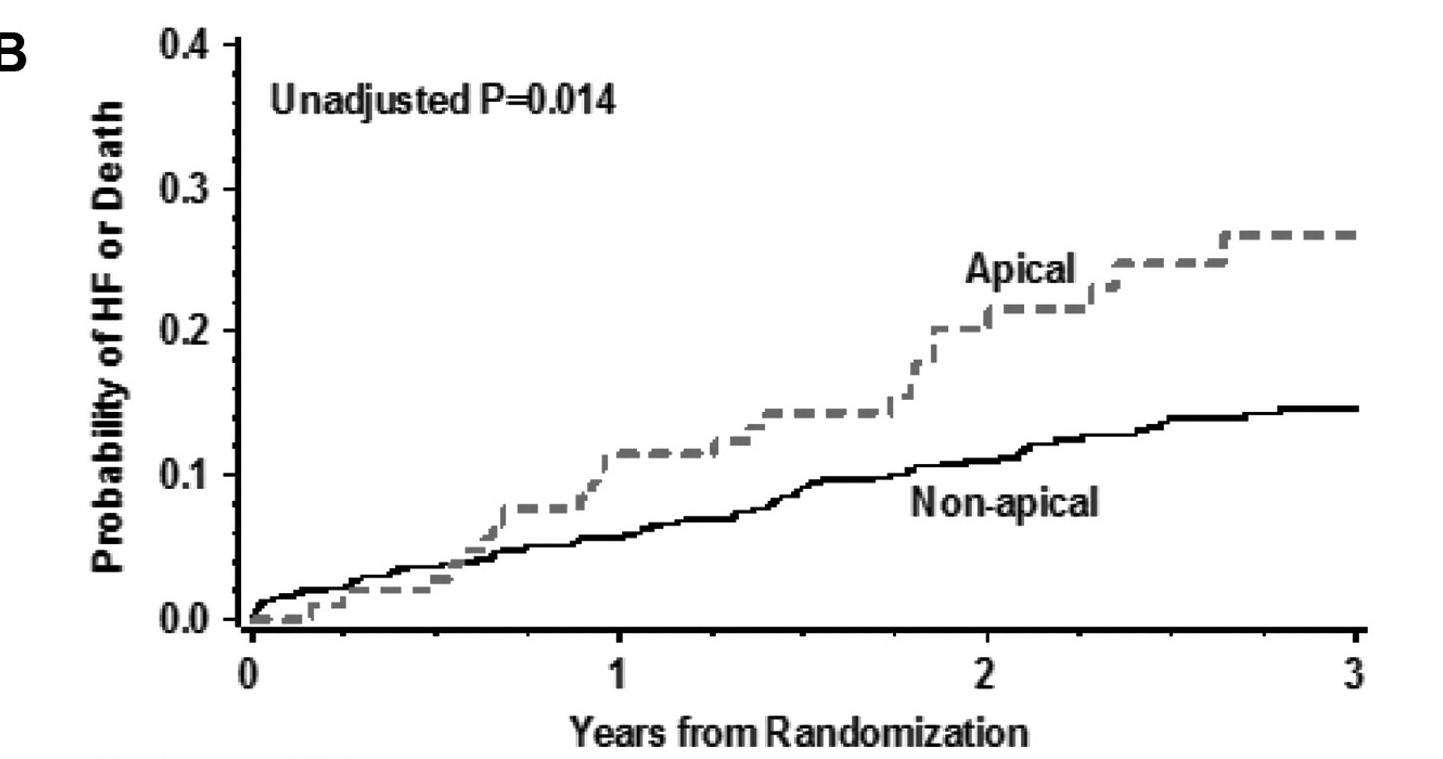
Singh JP, Klein HU, Huang DT, Reek S, Kuniss M, Quesada A, Barsheshet A, Cannom D, Goldenberg I, McNitt S, Daubert JP, Zareba W, Moss AJ. Left ventricular lead position and clinical outcome in the multicenter automatic defibrillator implantation trial-cardiac resynchronization therapy (MADIT-CRT) trial. Circulation. 2011 Mar 22;123(11):1159-66.
Miscellaneous
Anodal stimulation
- An easy to miss cause of non response
- Consider when using LV tip to RV coil / ring, dedicated bipolar leads and high output
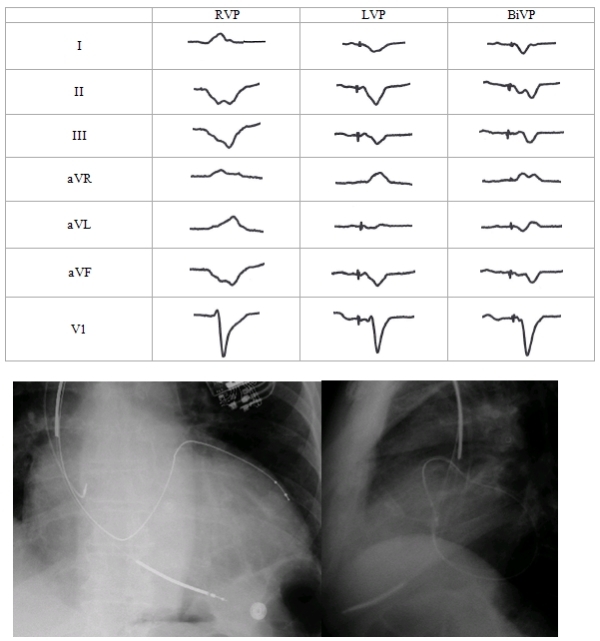
- Recognise by morphology of LV only pacing resembling RV pacing or fusion
Anodal stimulation
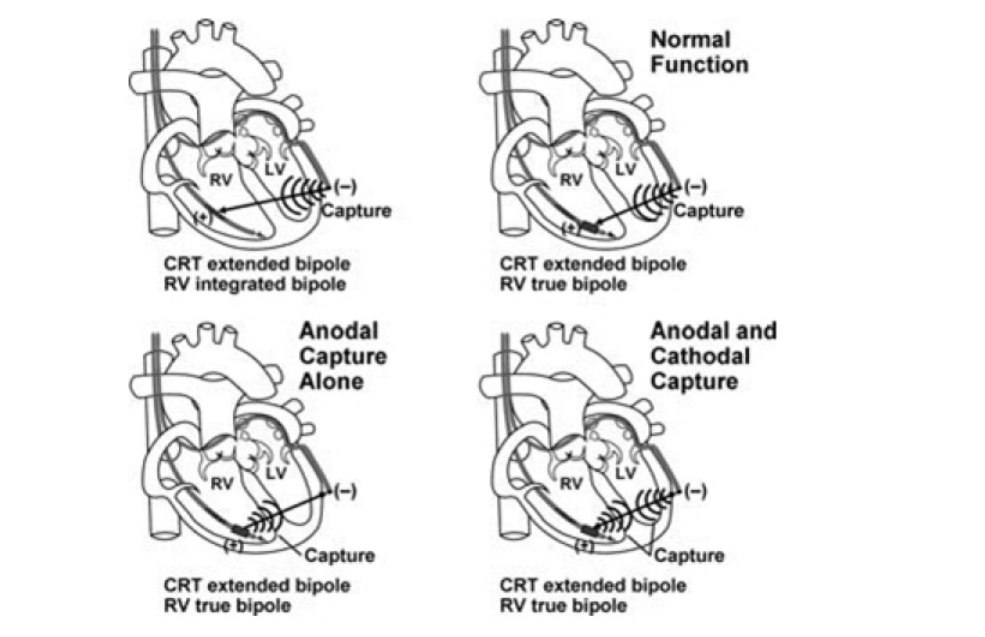
Anodal Stimulation: An Underrecognized Cause of Nonresponders to Cardiac Resynchronization Therapy
Khalin F Dendy, MD, Brian D Powell, MD, […], and Samuel J Asirvatham, MD. Indian Pacing Electrophysiol J. 2011 May-Jun; 11(3): 64–72.
Example
CRT optimization - Real world situation
- In real world, few do any optimization (1)
- In non responders, only small percentage improve with optimization
- Non response may indicate unfavourable substrate
Gras D, Gupta MS, Boulogne E, Guzzo L, Abraham WT. Optimization of AV and VV delays in the real-world CRT patient population: an international survey on current clinical practice. Pacing Clin Electrophysiol. 2009 Mar;32 Suppl 1:S236-9.
Other management options
- Multisite pacing
- Multipoint pacing
- LV endocardial pacing
- Conduction system pacing
Summary
- Empiric programming at implant sufficient
- Assess for response at 3-6 months
- Partial and non responders - attempt optimization guided by ECG and Echo
- Role for device based optimization algorithms is small
- Low threshold for AVJ ablation in AF
- Consider anodal stimulation in appropriate settings