Diagnosis and Treatment of Patients With Hypertrophic Cardiomyopathy

Guidelines
- 34 year old male
- Chest pain - abnormal ECG, evaluation suggestive of HCM, referred
- DOE class II NYHA
Recommended initial evaluation
- Clinical examination (1, B-NR)
- 12 lead ECG (1, B-NR)
- Echocardiogram (1, B-NR)
- 24 to 48 hour ambulatory ECG monitoring (1, B-NR)
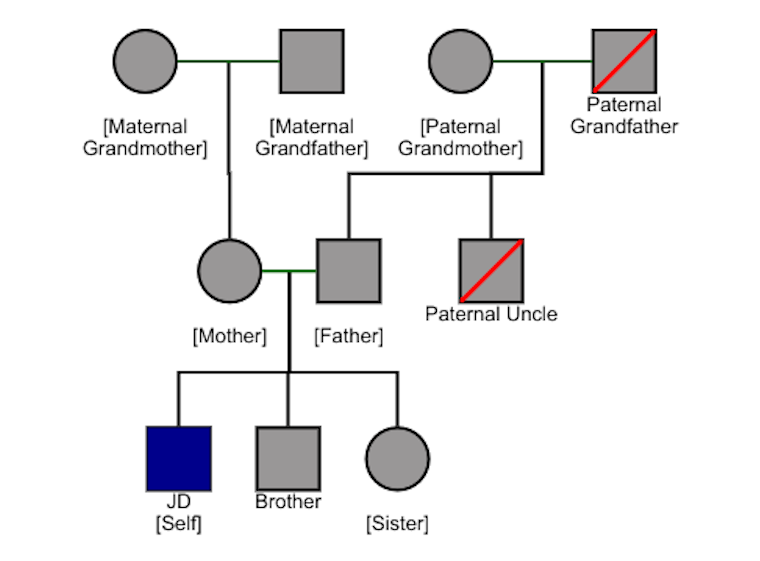
Family history
Echocardiogram
- Left ventricular hypertrophy
- IVS 18 mm - thickest part of LV
- Outflow gradient - 24 mm Hg
- LVEF 65%
- No apical aneurysm
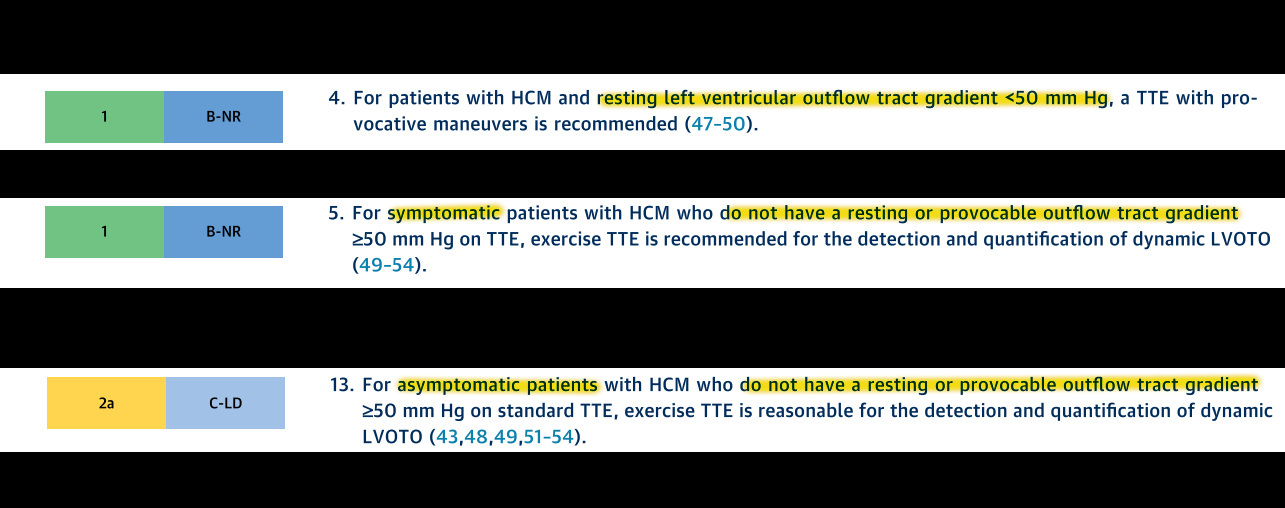
Echocardiogram - Questions
- Provocative maneuvers?
- Exercise
- Echo contrast ?
- TEE ?
Provocative maneuvers / Exercise
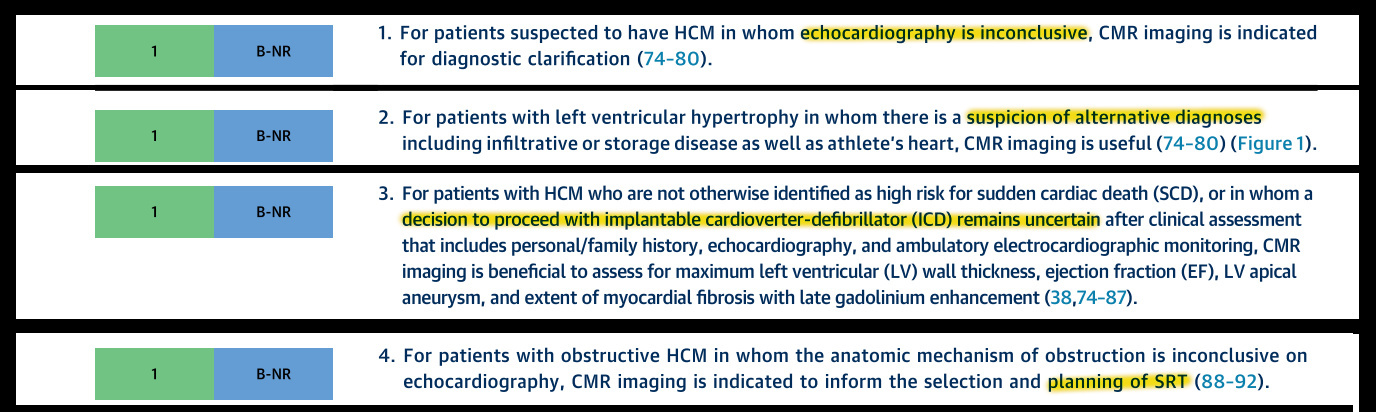
CMR
- When is it needed ?
- What information does it provide ?
- CT is an alternative if CMR not available (2b, C-LD)
CMR
Heart Rhythm assessment
- 12 lead ECG (1, B-NR)- Left ventricular hypertrophy
- 24 hr Ambulatory ECG (1, B-NR) - No arrhythmias
- Event recorders in case of symptoms to document rhythm correlation (1, B-NR)
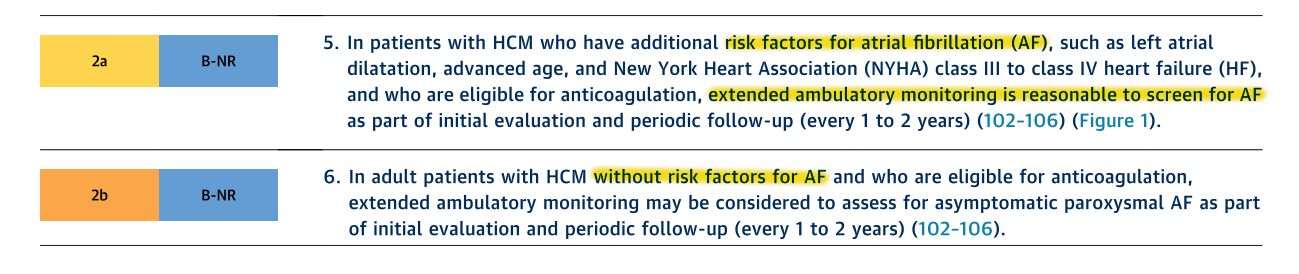
Screening for AF
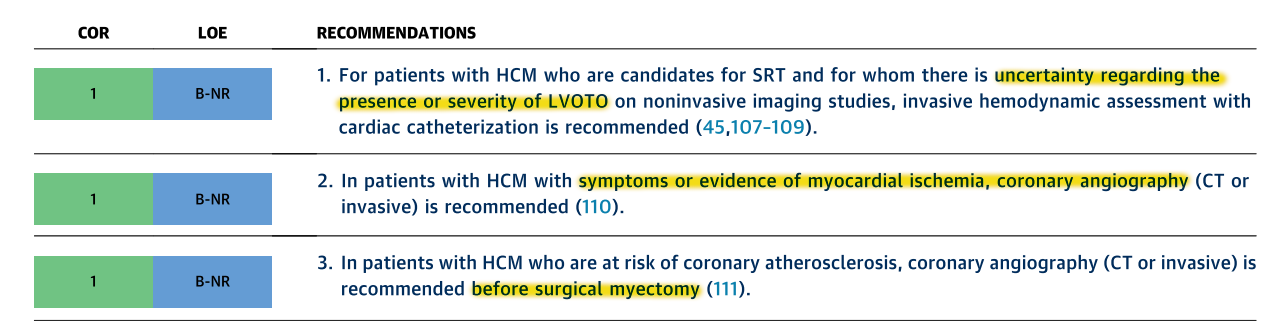
Cath / Angiography ?
- Completed clinical evaluation
- Echo / ECG / Holter
- CMR / AECG
- Genetic testing ?
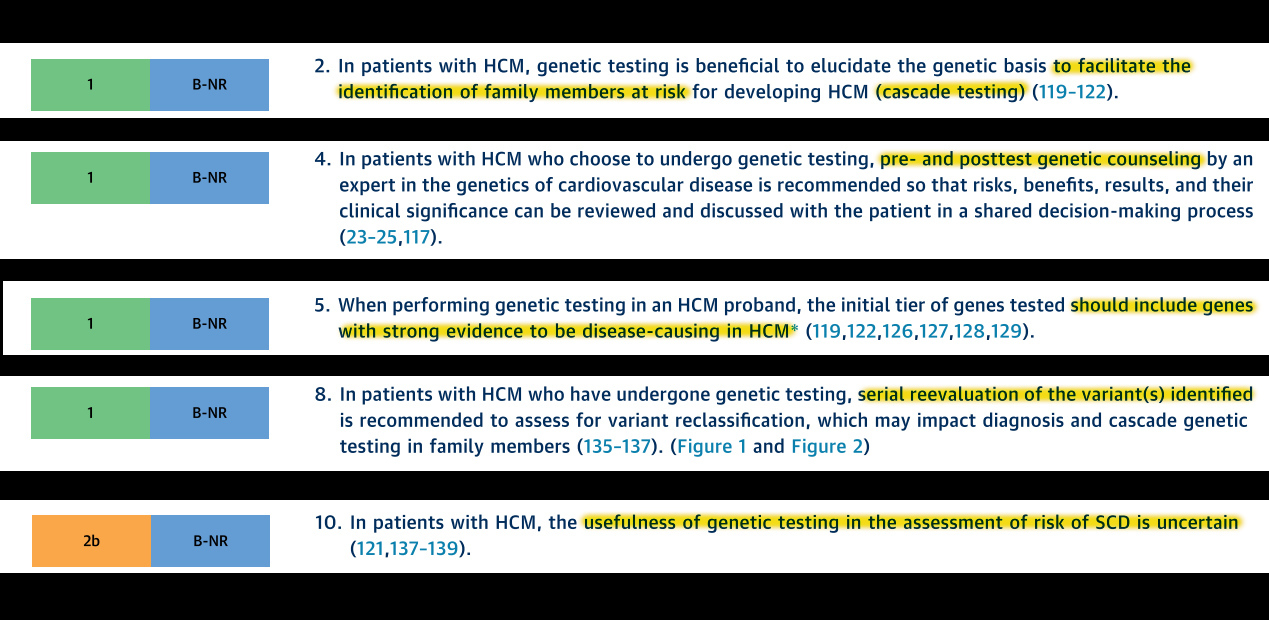
Genetic testing
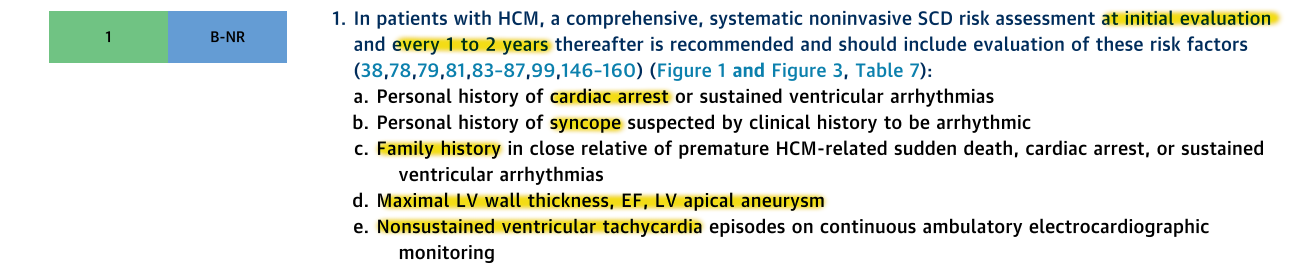
SCD evaluation - Essential
SCD - Optional evaluation
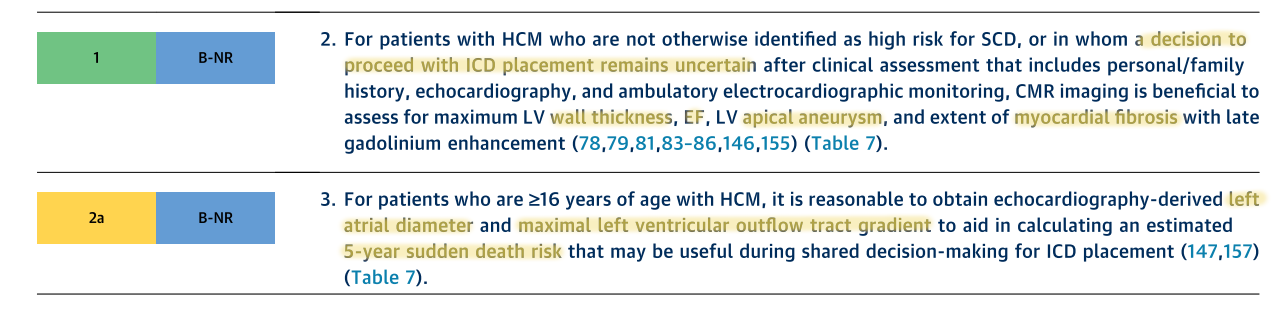
SCD - Risk factors
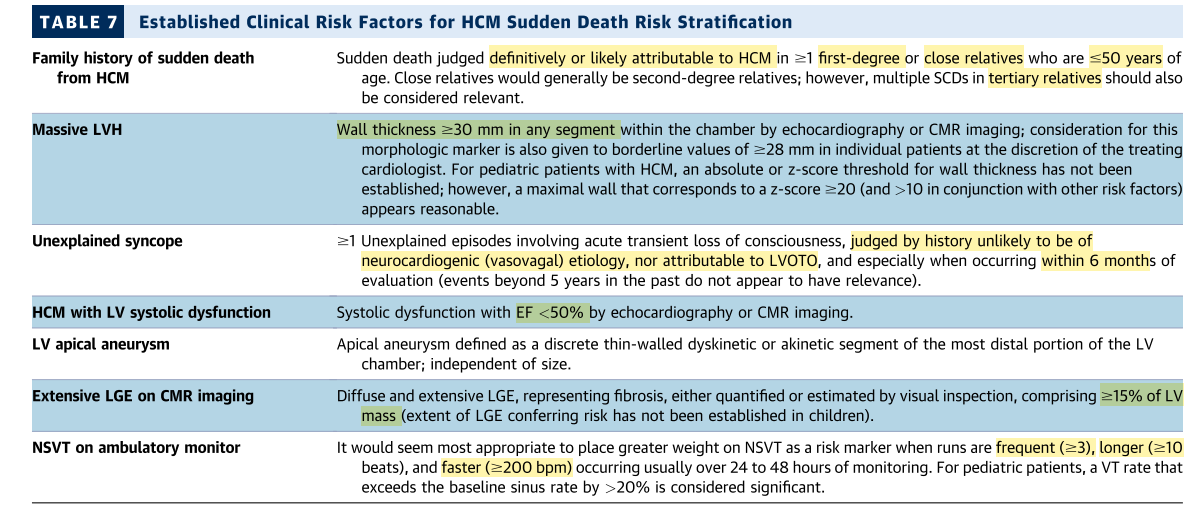
5 year SCD risk assessment
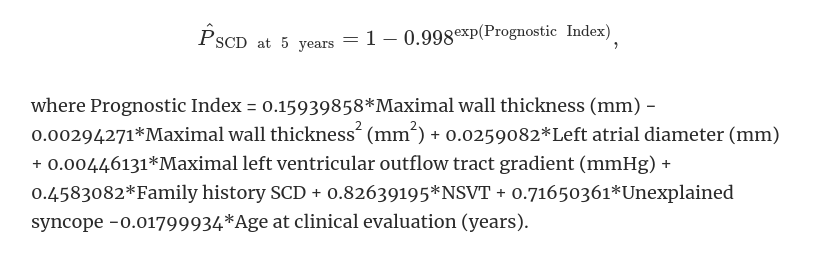
Constantinos O'Mahony et al, for the Hypertrophic Cardiomyopathy Outcomes Investigators, A novel clinical risk prediction model for sudden cardiac death in hypertrophic cardiomyopathy (HCM Risk-SCD), European Heart Journal, Volume 35, Issue 30, 7 August 2014, Pages 2010–2020
Review of our patients risk - Does he need an ICD ?
- No previous cardiac arrest / sustained VT
- Sudden death in close relative < 50 yrs
- LVH not > 30 mm
- No arrhythmic syncope recently
- No LV apical aneurysm
- Normal LVEF
Shared decision making
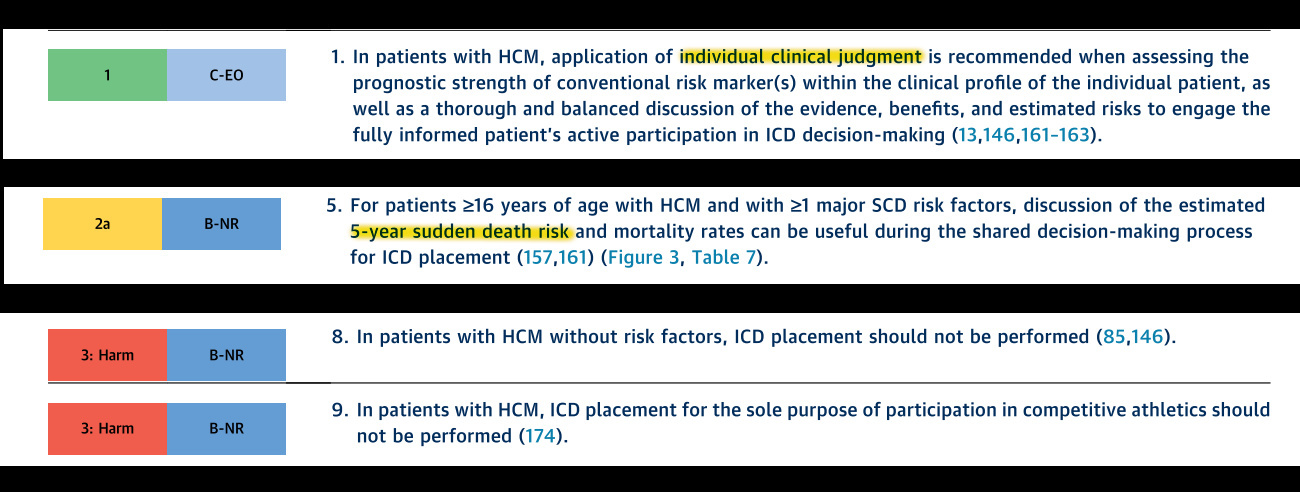
Decision
- Young age, dependent family
- Family history of sudden death
- Decided to undergo ICD implant
- CMR could have helped if undecided
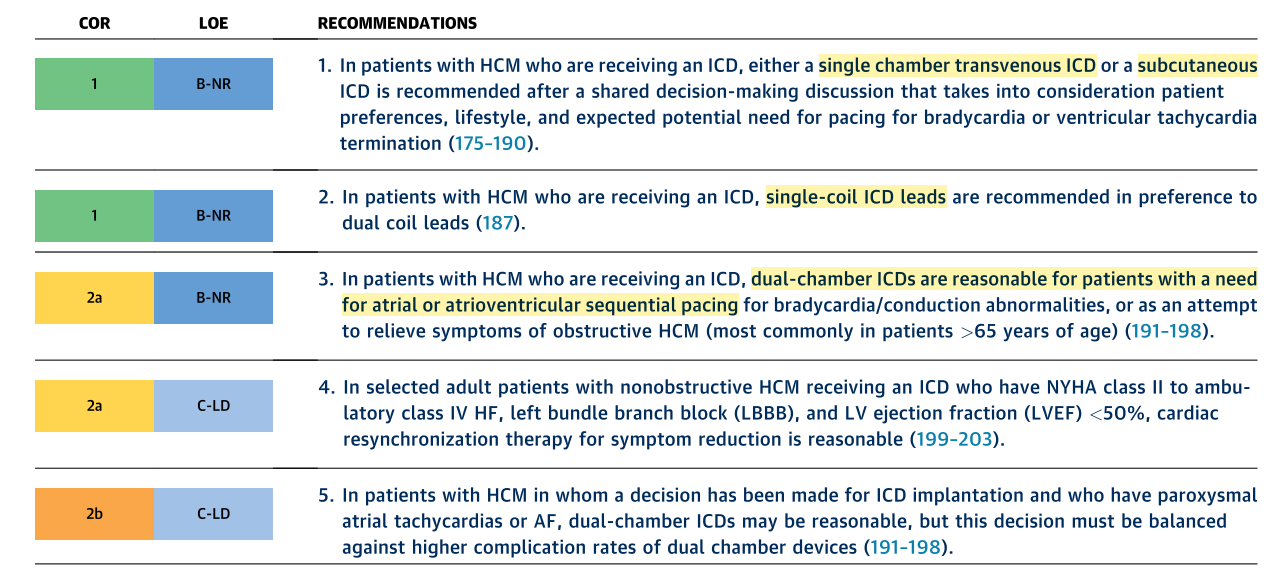
Which ICD ?
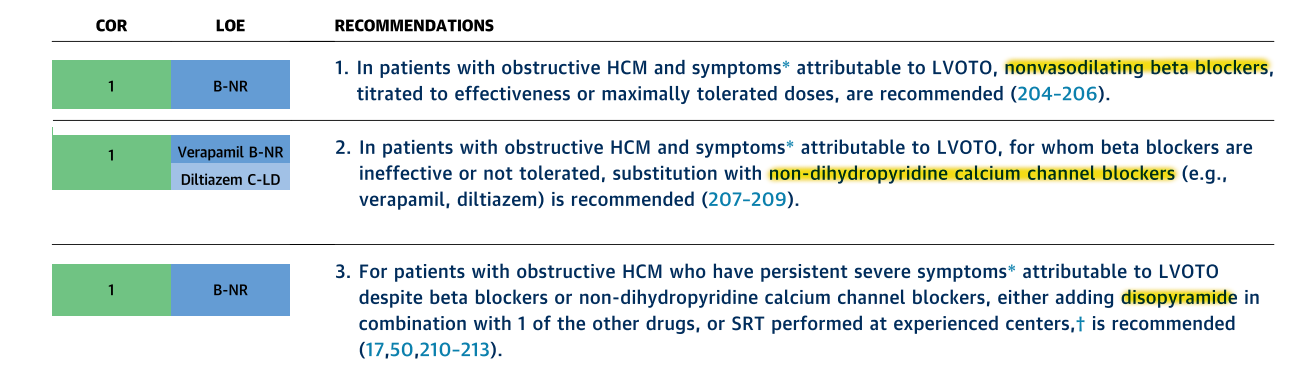
Pharmacologic management - Obstructive HCM
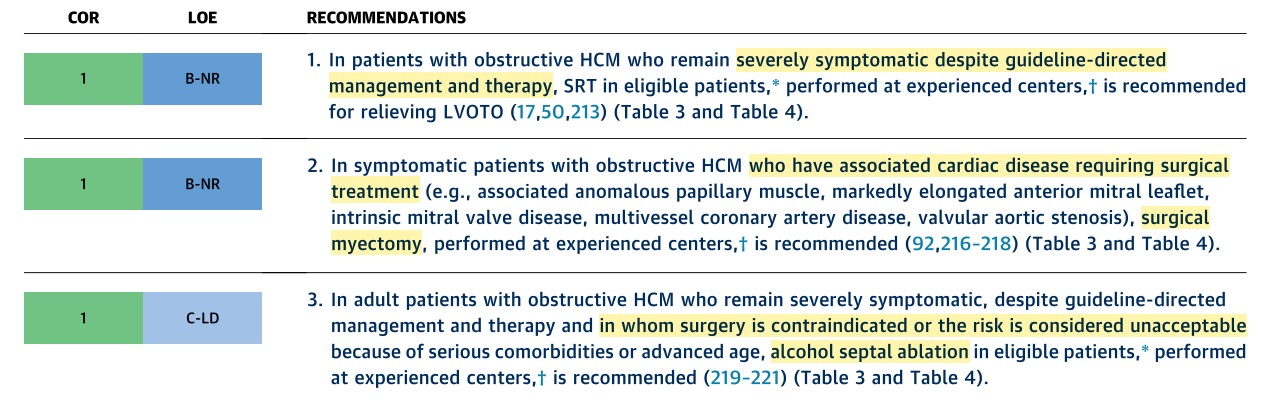
Septal reduction therapy
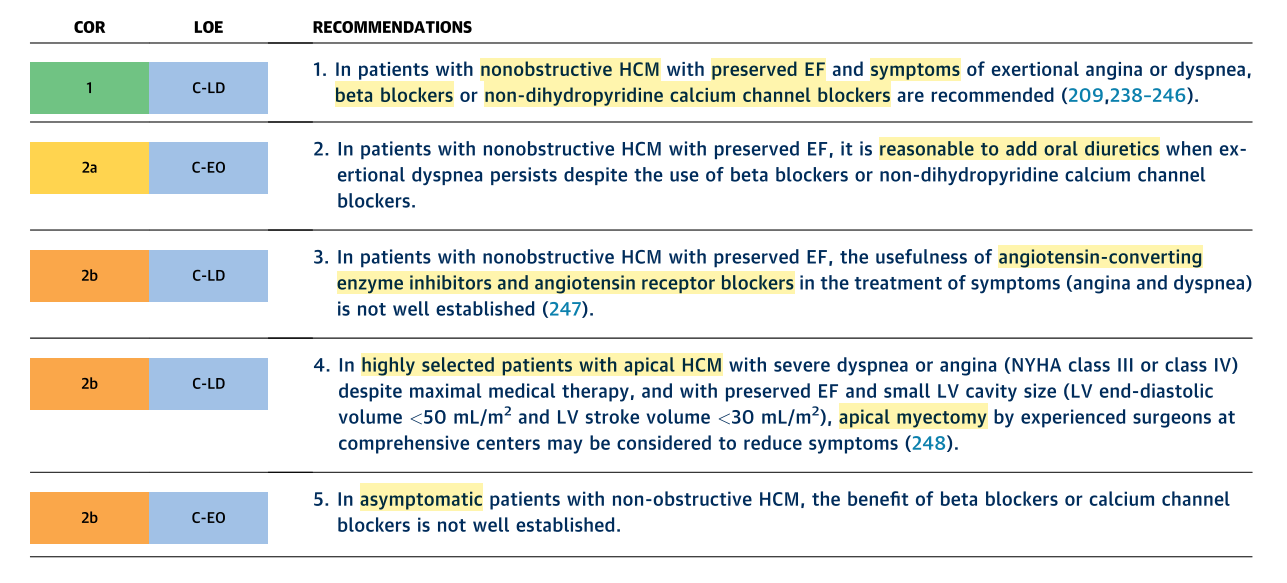
Pharmacologic management - Non obstructive HCM
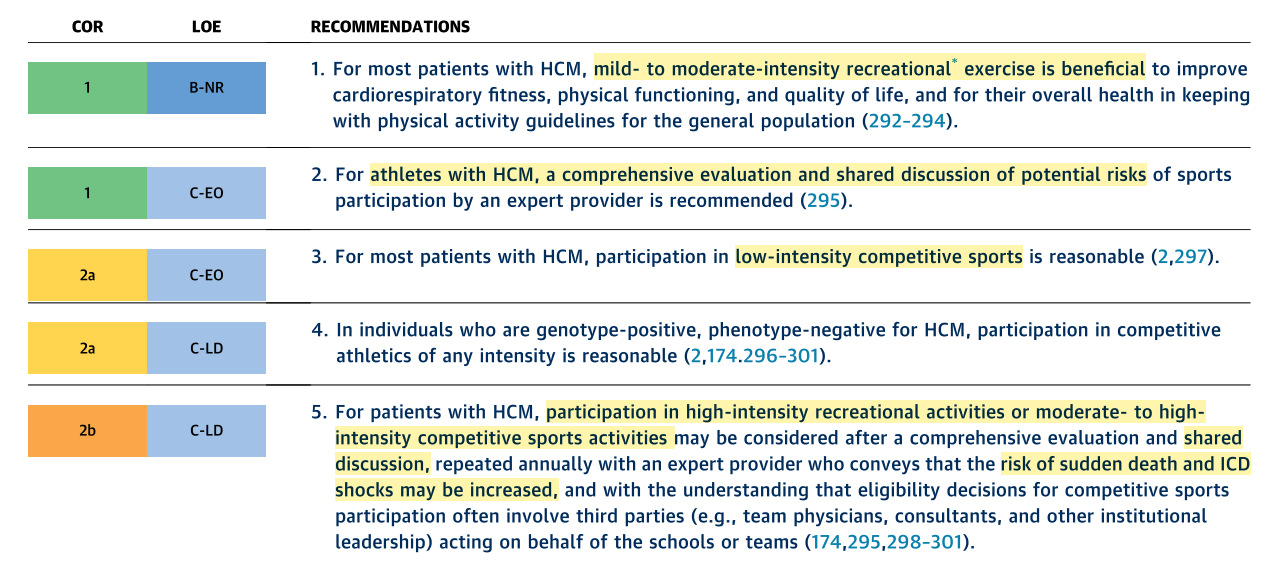
Lifestyle - Sports and activity
Outcome of evaluation and prescription
- Non-obstructive HCM, NYHA II
- SCD risk (one risk factor) - Single chamber ICD
- Drugs - beta blocker
- Screening of family members
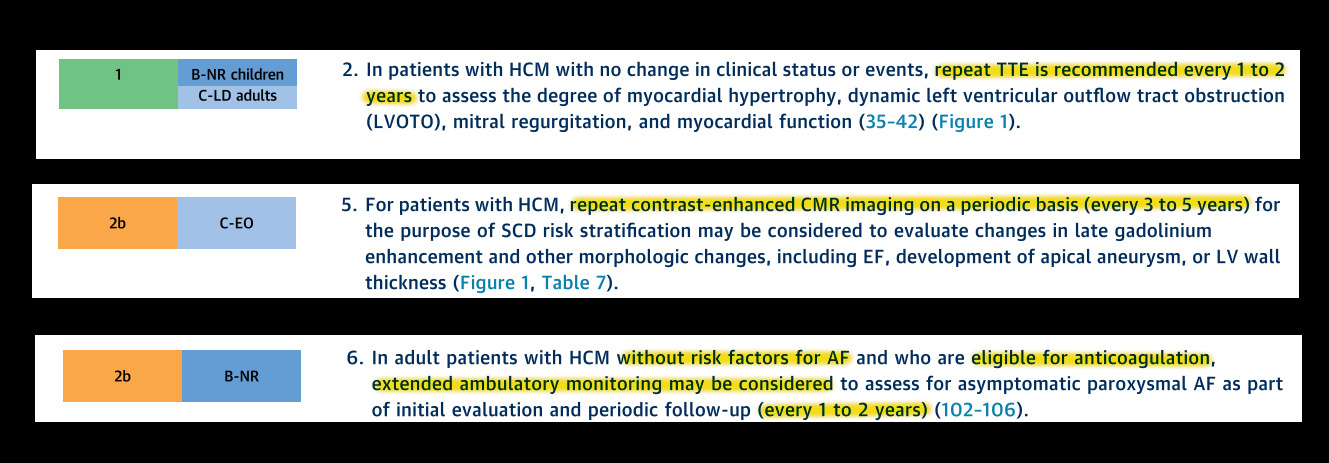
- Periodic evaluation schedule
Follow up schedule
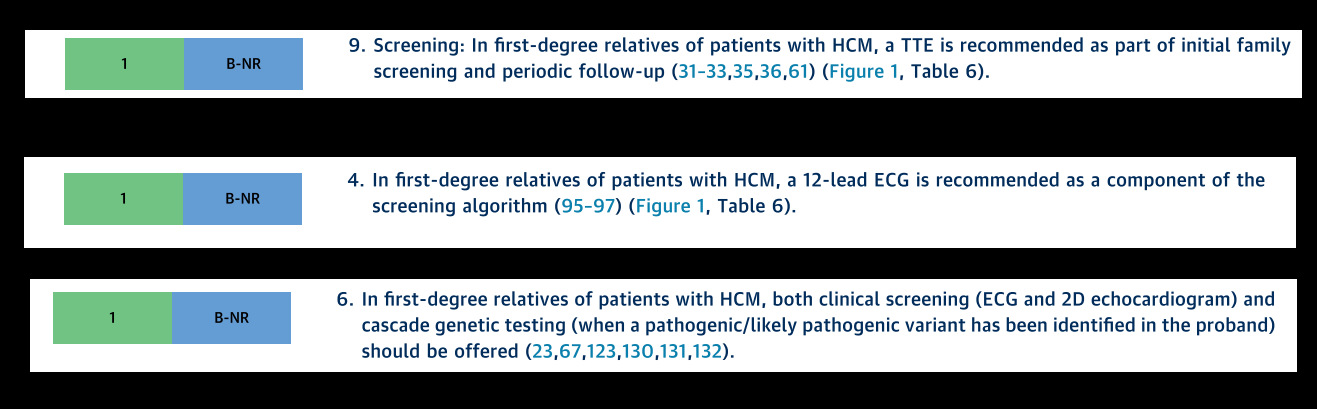
Family screening
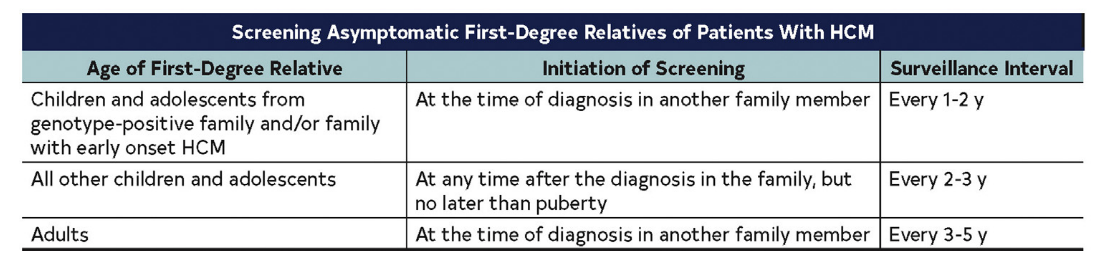
Family screening
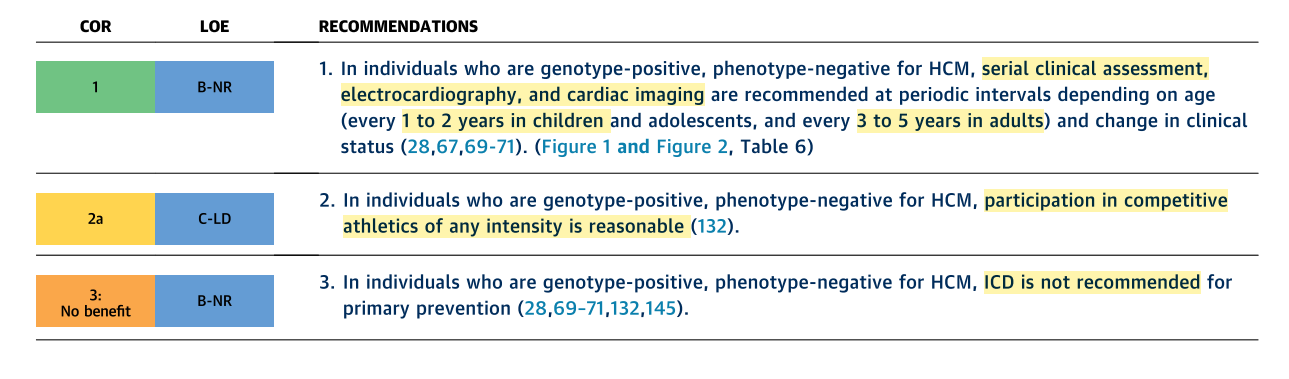
Genotype positive, phenotype negative
Six months later - Acute breathlessness
- AF ecg
- Paroxysmal AF
- CHADS-VASC 0 - OAC or not ?
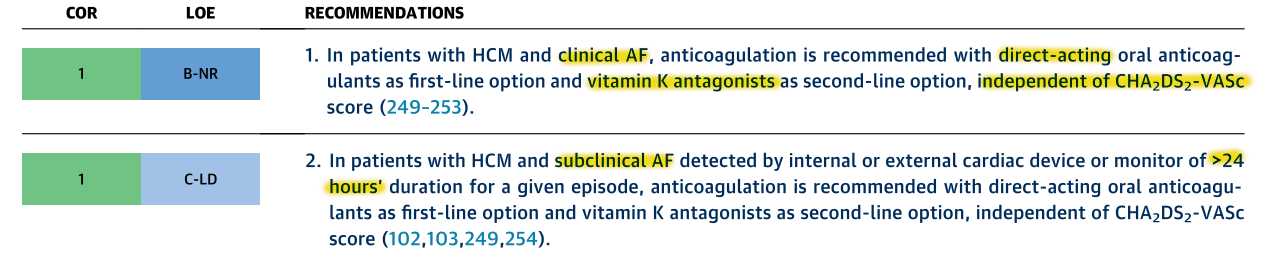
Anticoagulation for AF
Top take home messages
- Imaging plays a crucial role in care, Echo remains most important, MRI useful in many patients
- Assessment of individual patient's risk continues to evolve
- Septal reduction therapies continue to improve in efficacy and safety
- In patients with AF, anticoagulant therapy needed irrespective of CHADS-VASC score
- EF < 50 indicates significant dysfunction and higher risk
- Moderate exercise is beneficial