
Rules
- Do not ablate without making a diagnosis
- Do not ablate without mapping completely
- Do not ablate unless you are sure you can recognize and avoid AV block
- Except specific situations, high power ablation does not succeed where low power fails
- Do not ablate for cosmetic reasons
Diagnosis
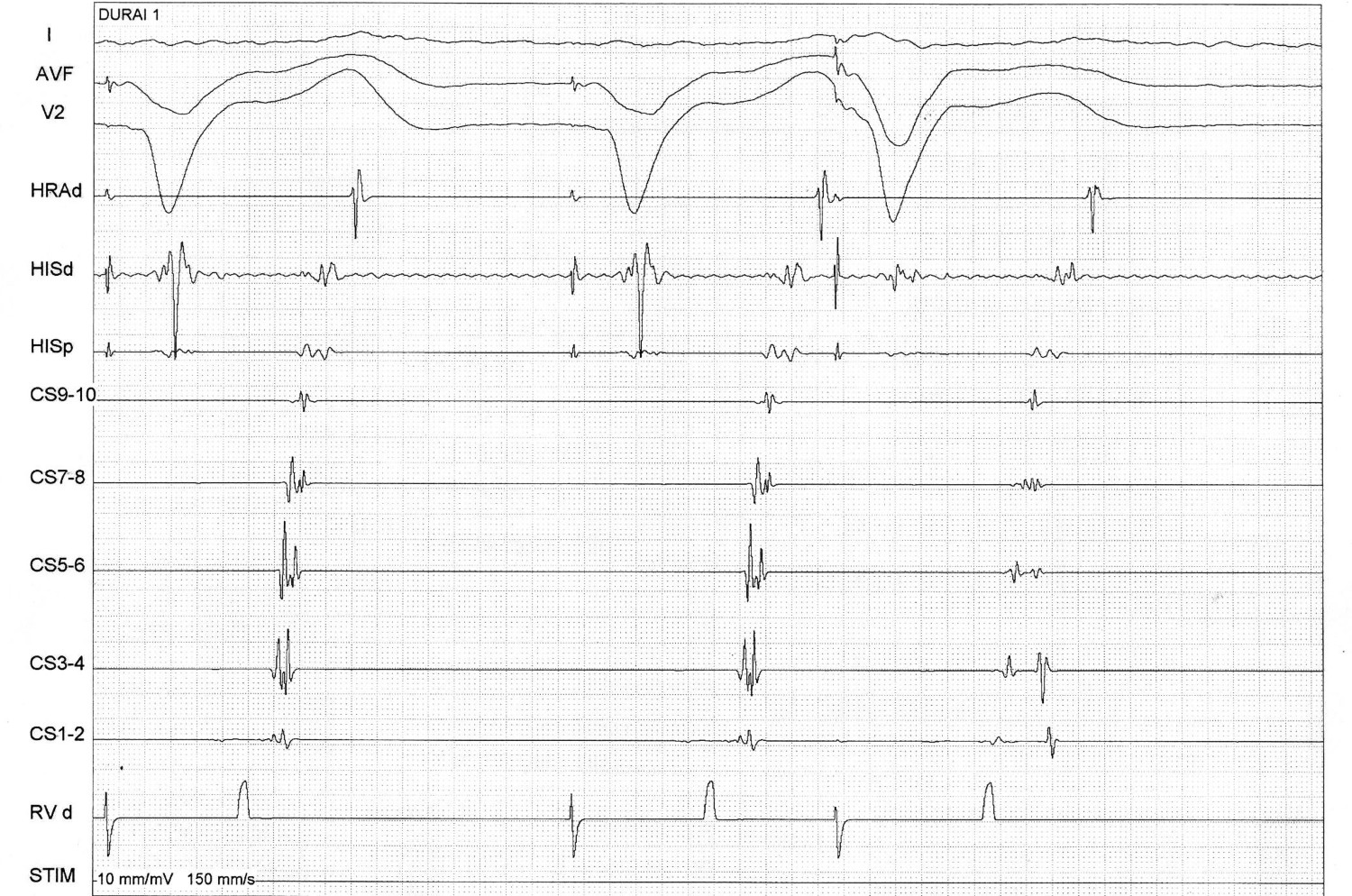
Dont skip the RA catheter
Dont skip the RA catheter

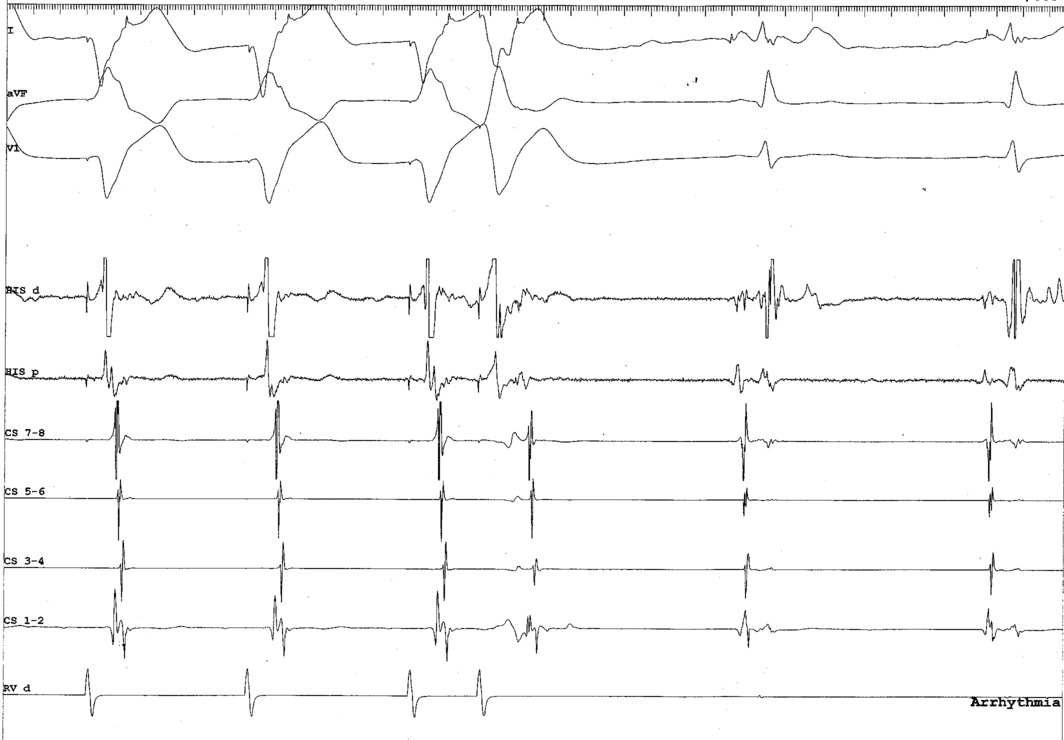
RV catheter at base
Mapping
Use triggered mode
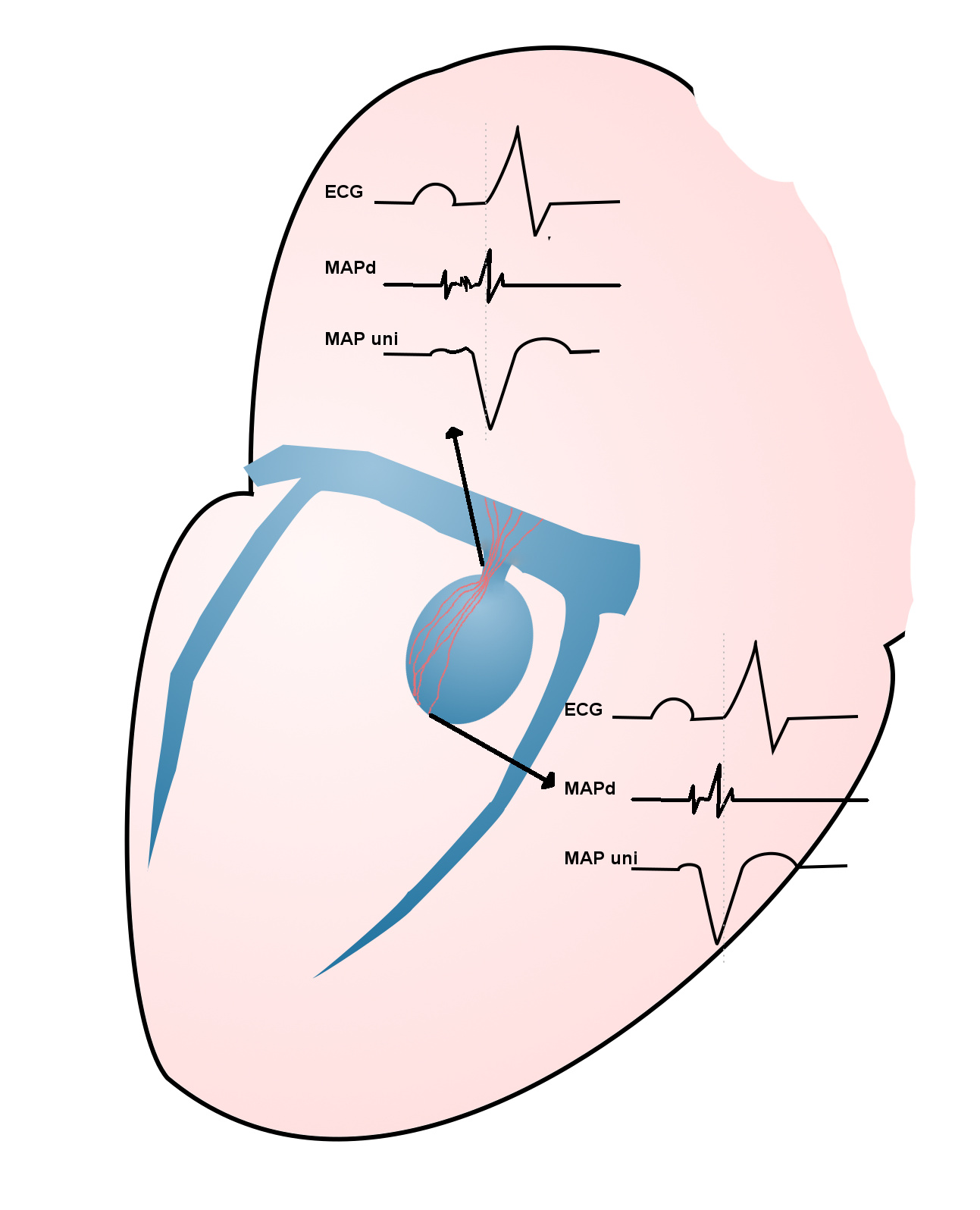
Use unipolar EGMs

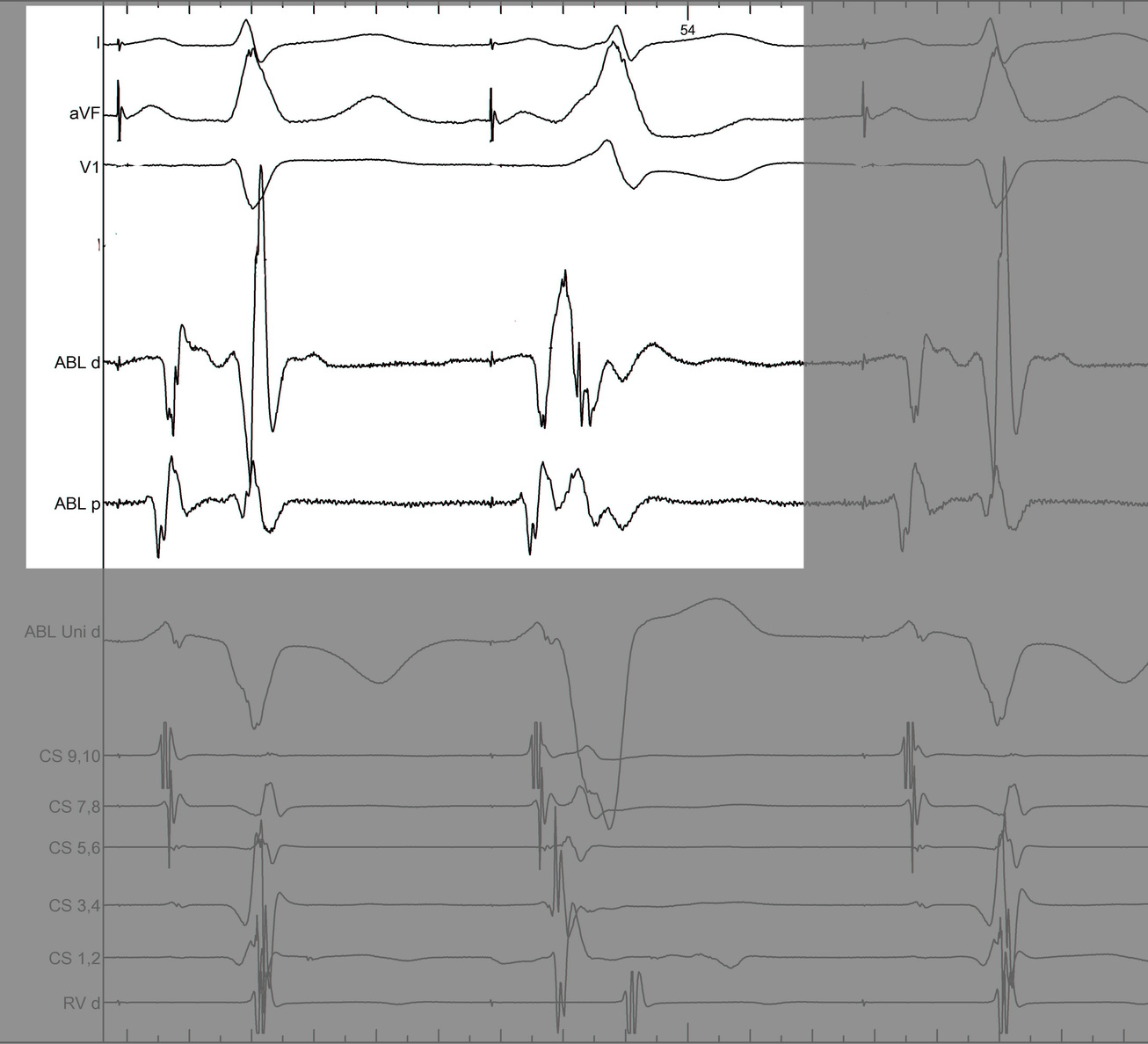
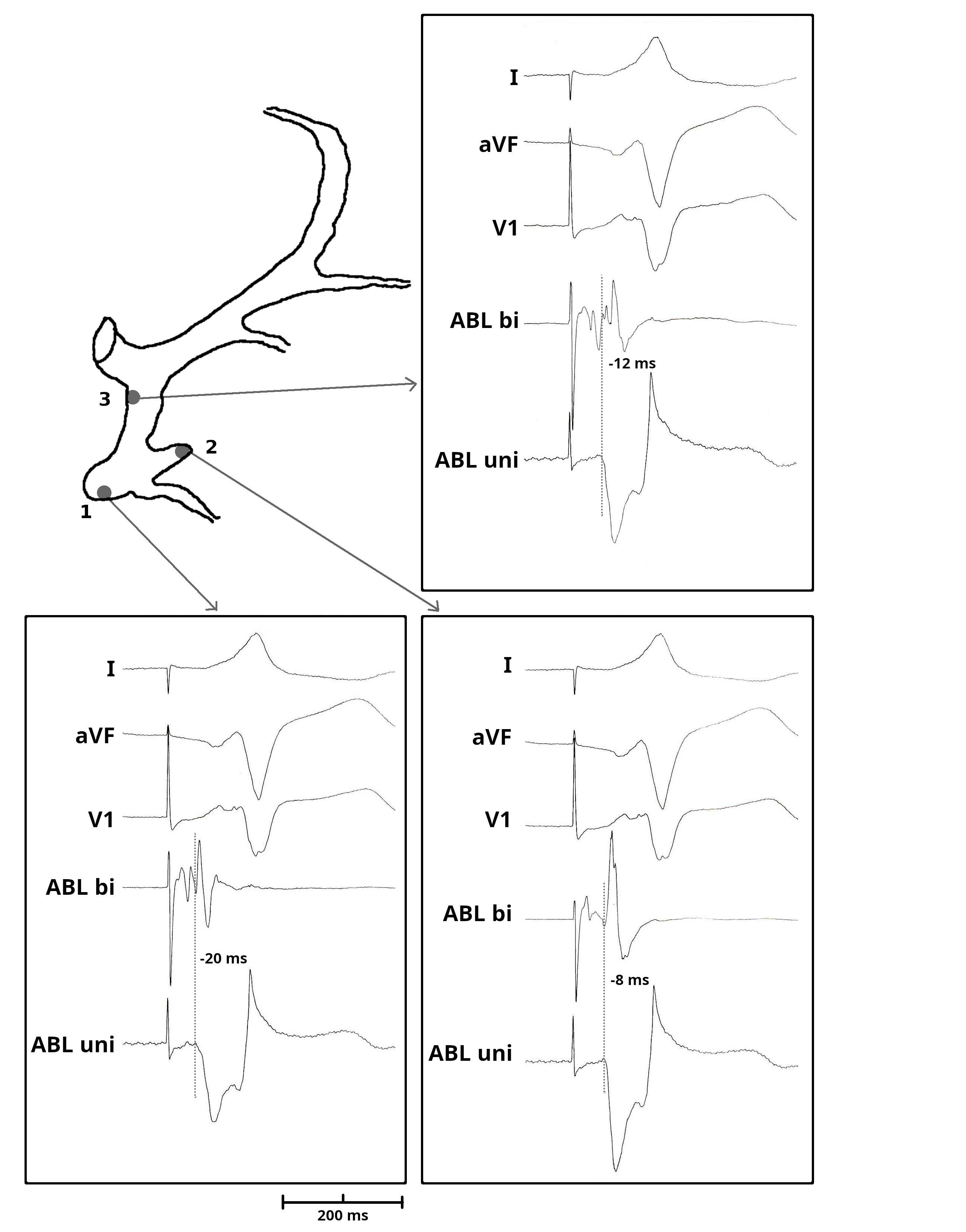
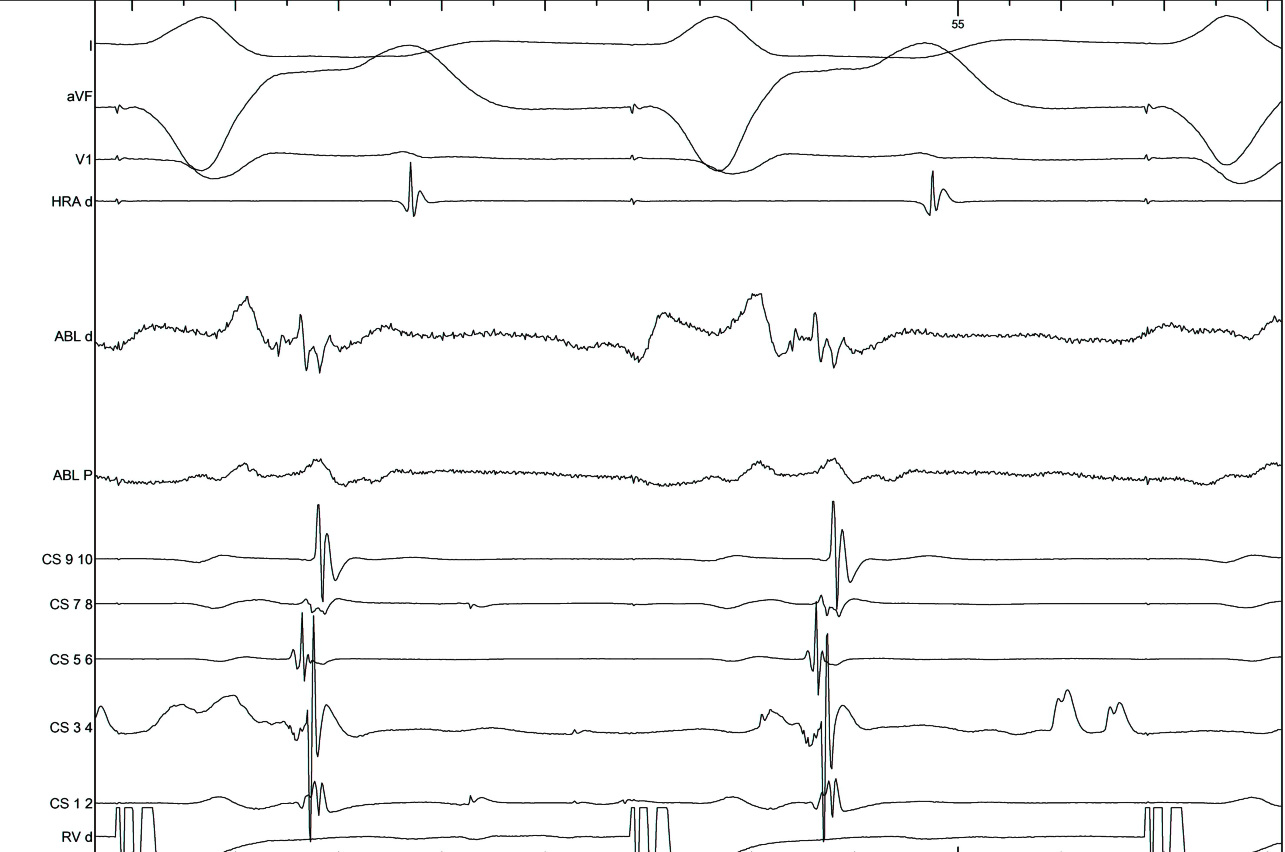
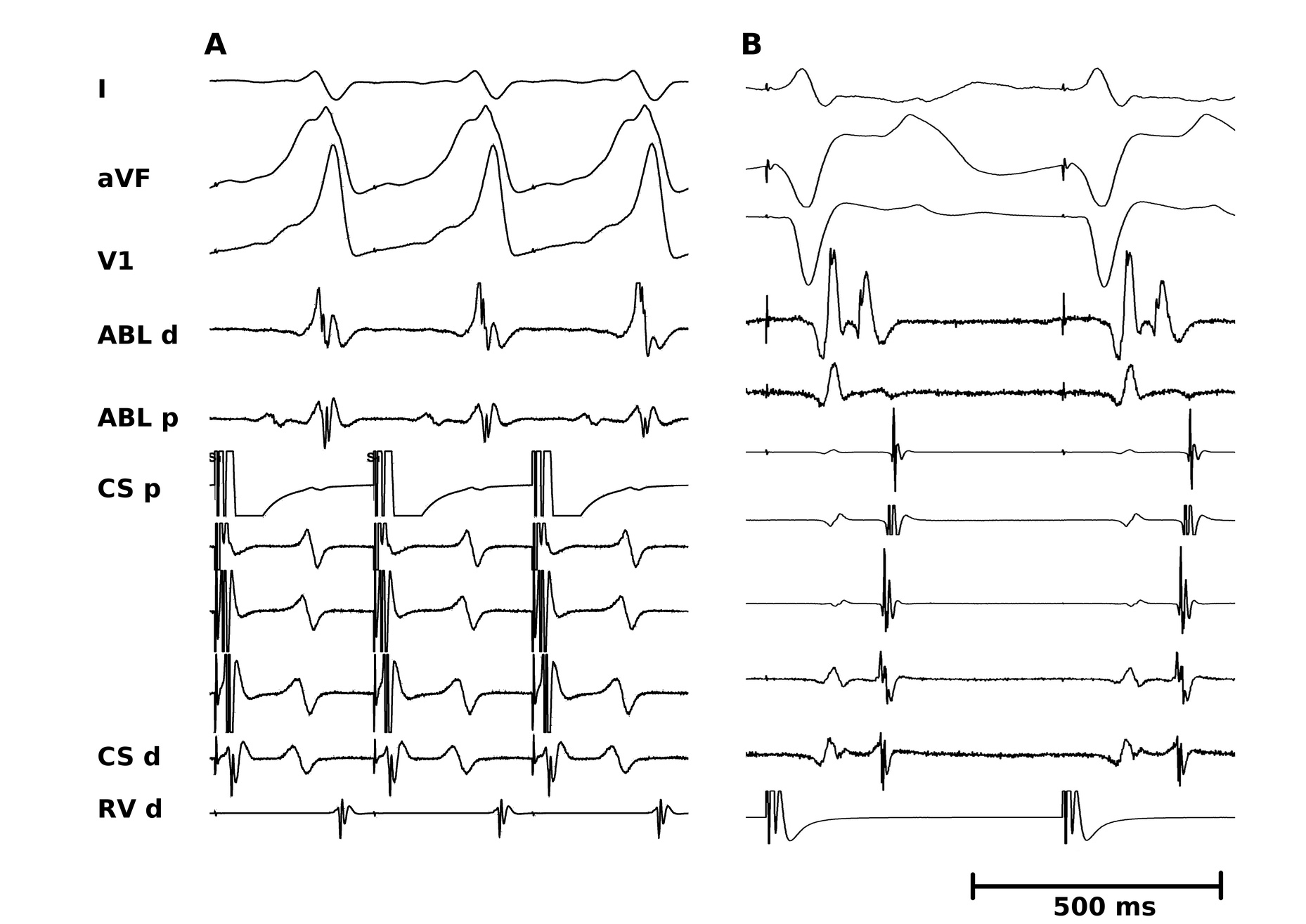
Identify components of the signal
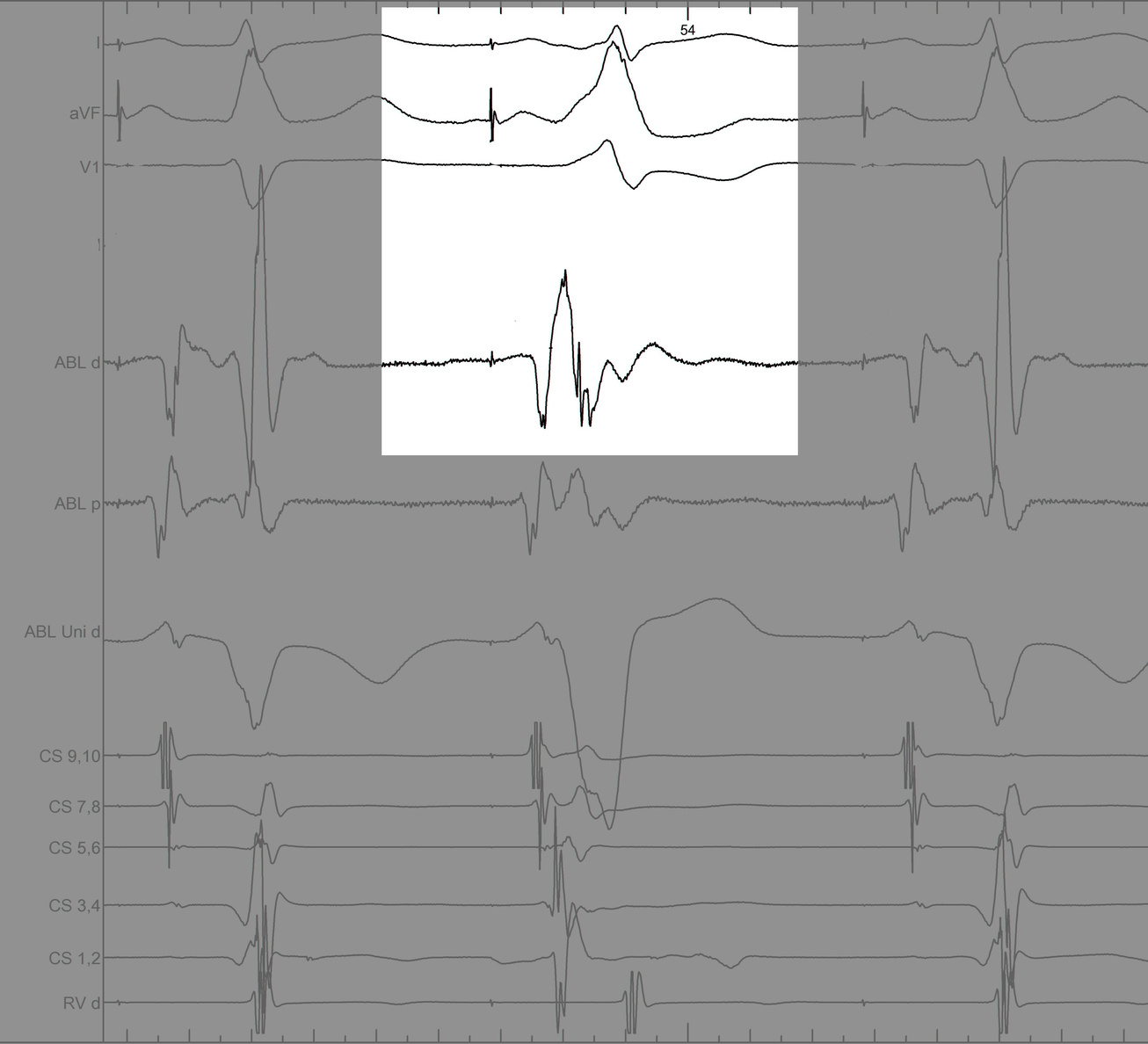
Identify components of the signal
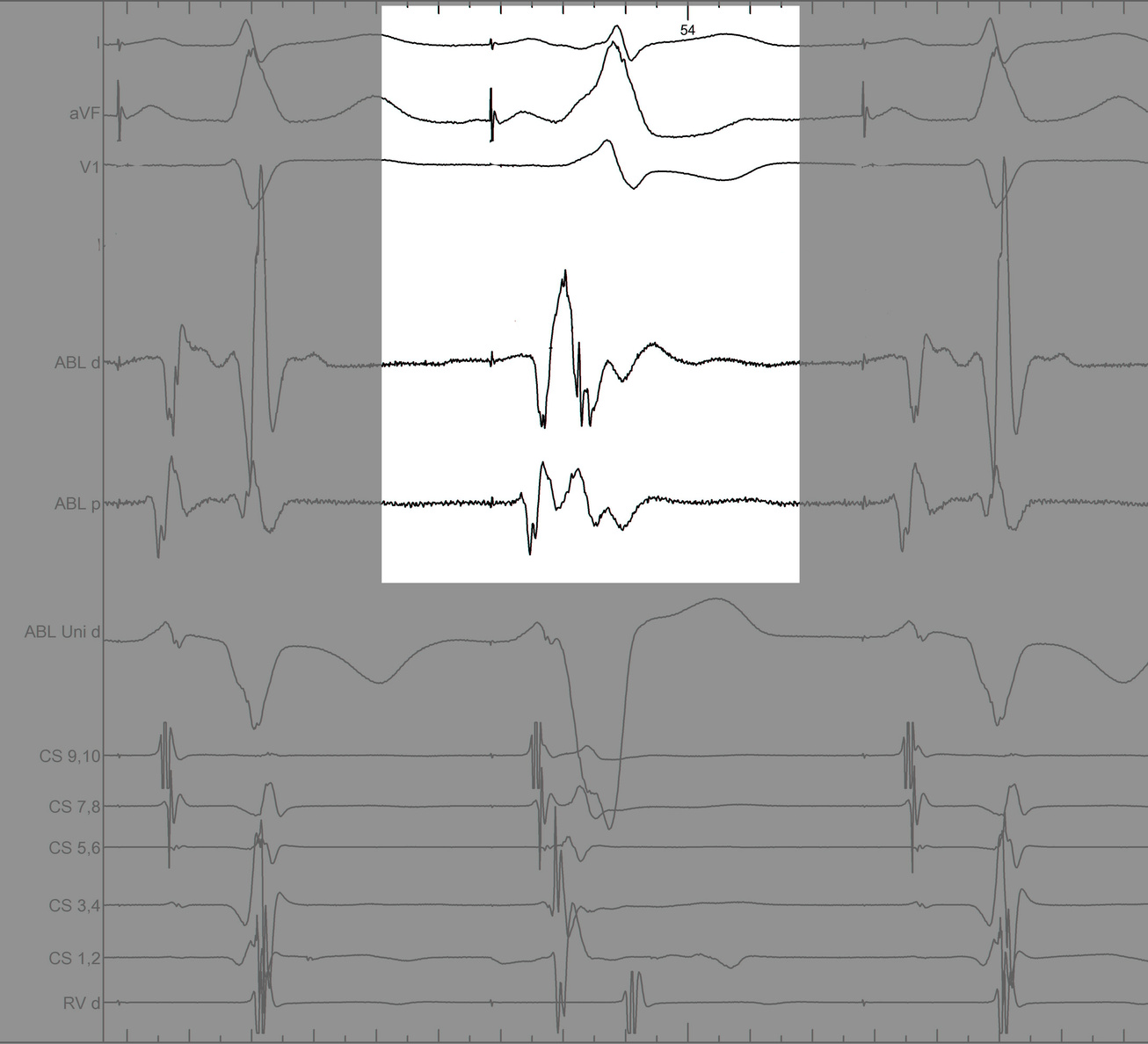
Identify components of the signal
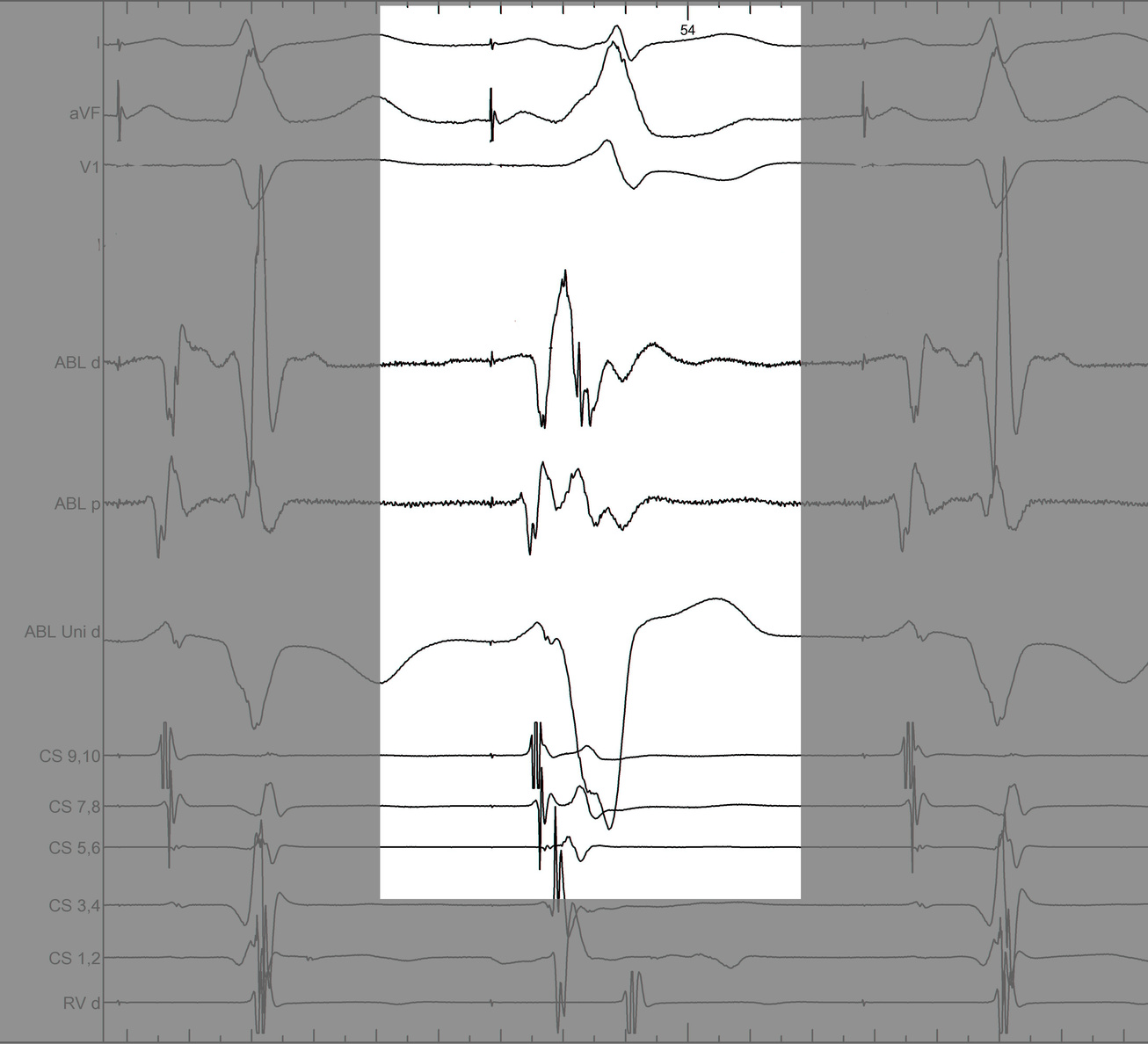
Identify components of the signal
LA-CS potential to identify endocardial / epicardial
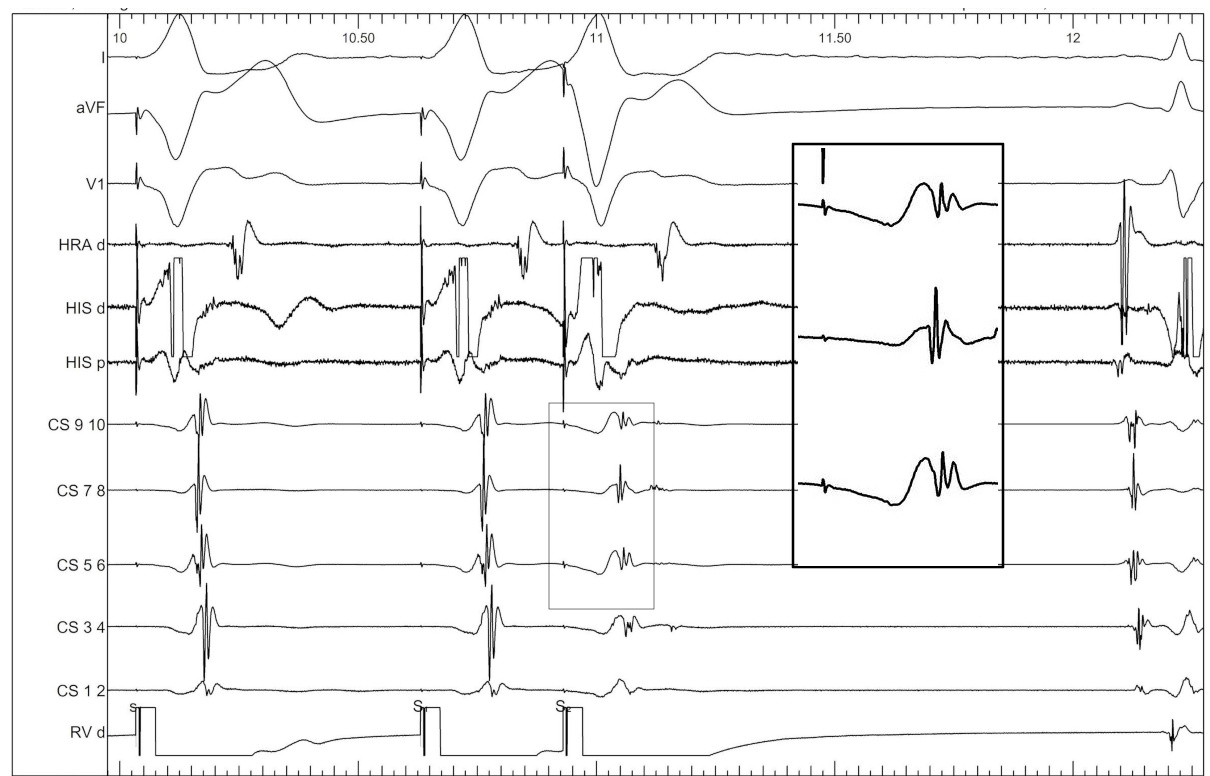
LA-CS potential to identify endocardial / epicardial
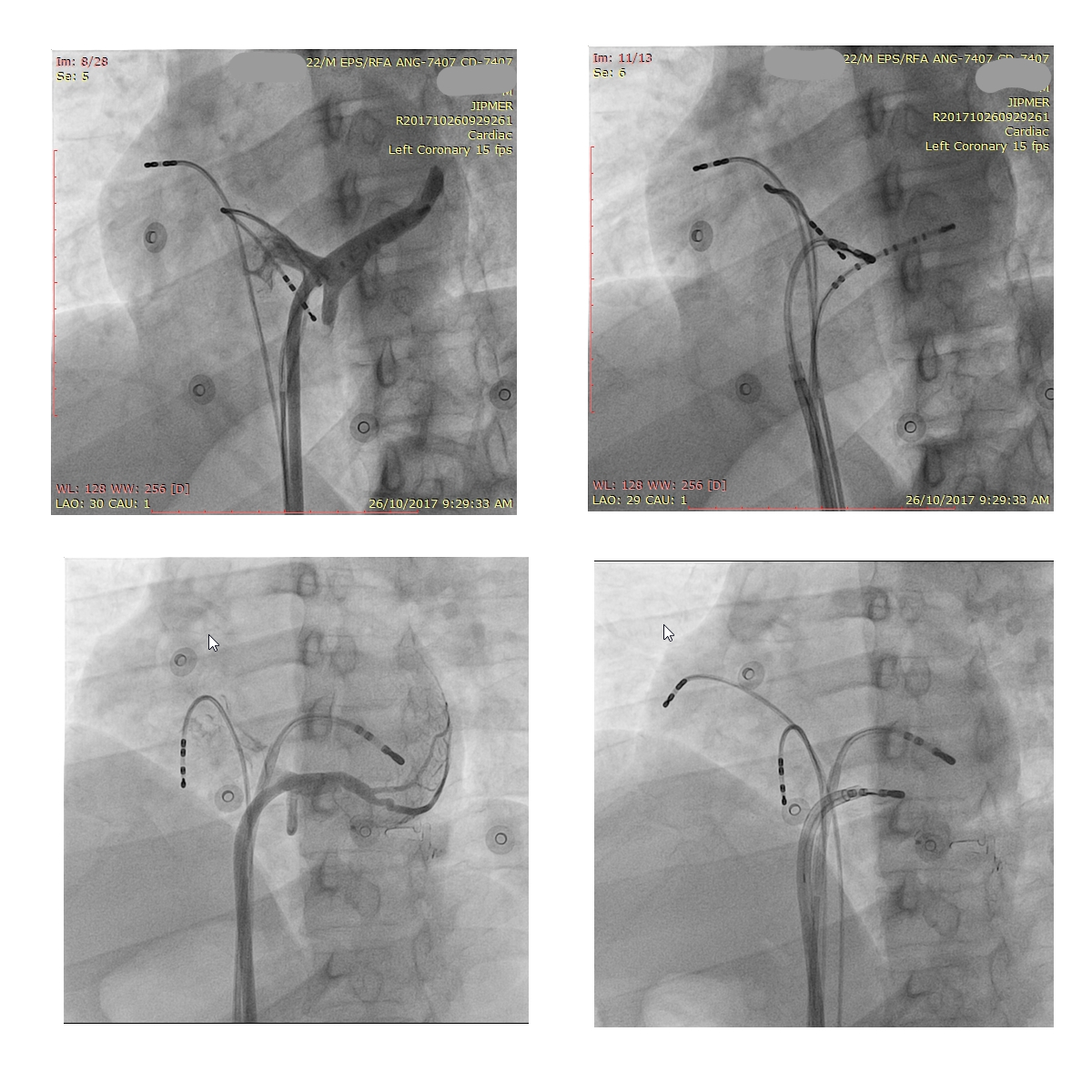
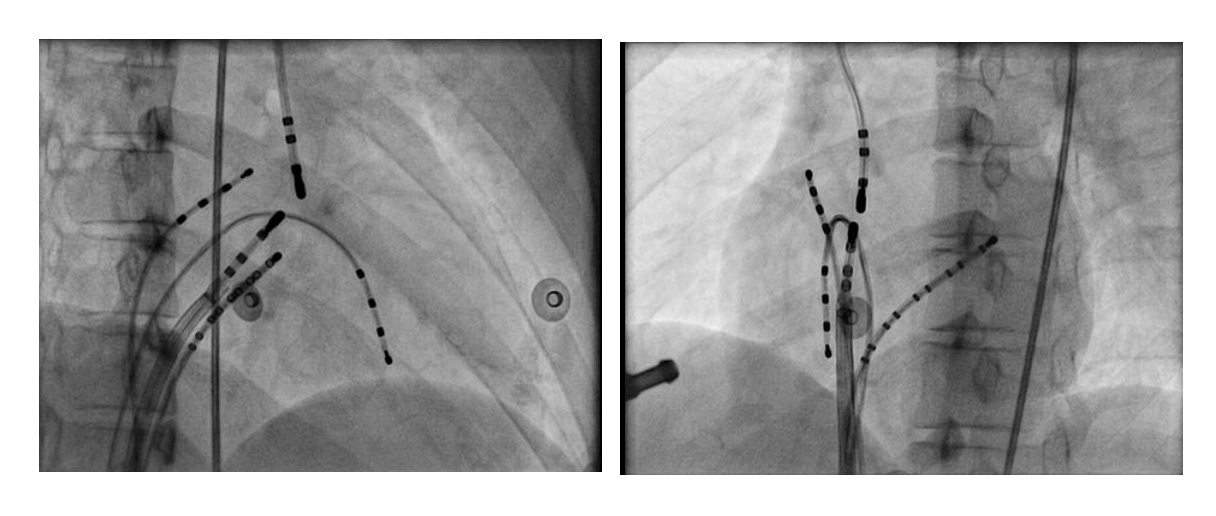
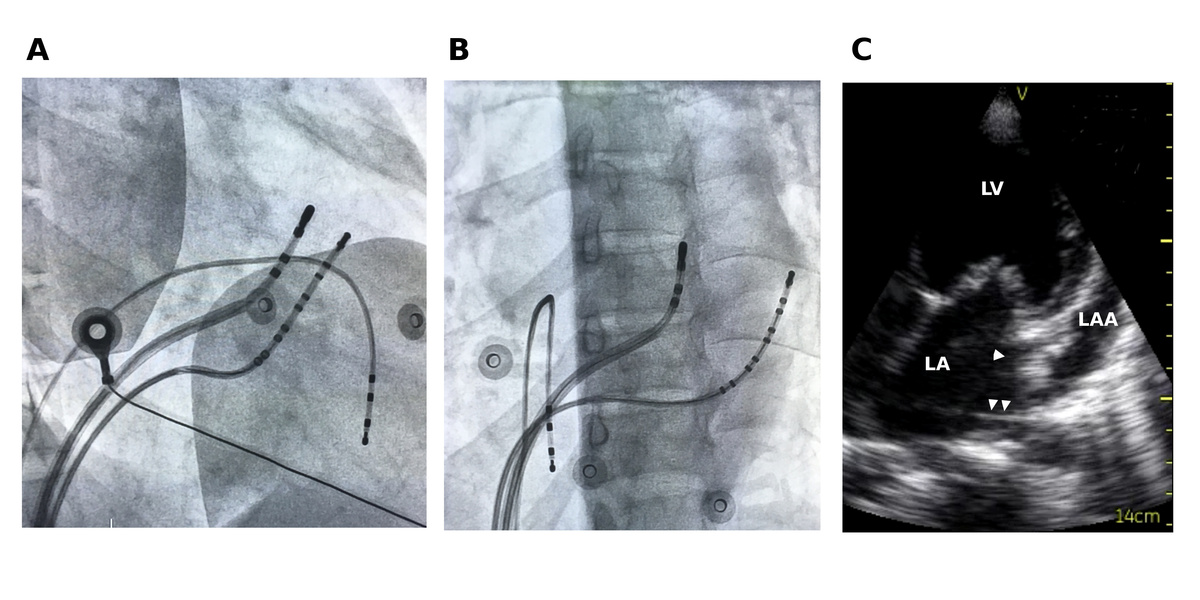
CS diverticulum
Mapping in diverticulum
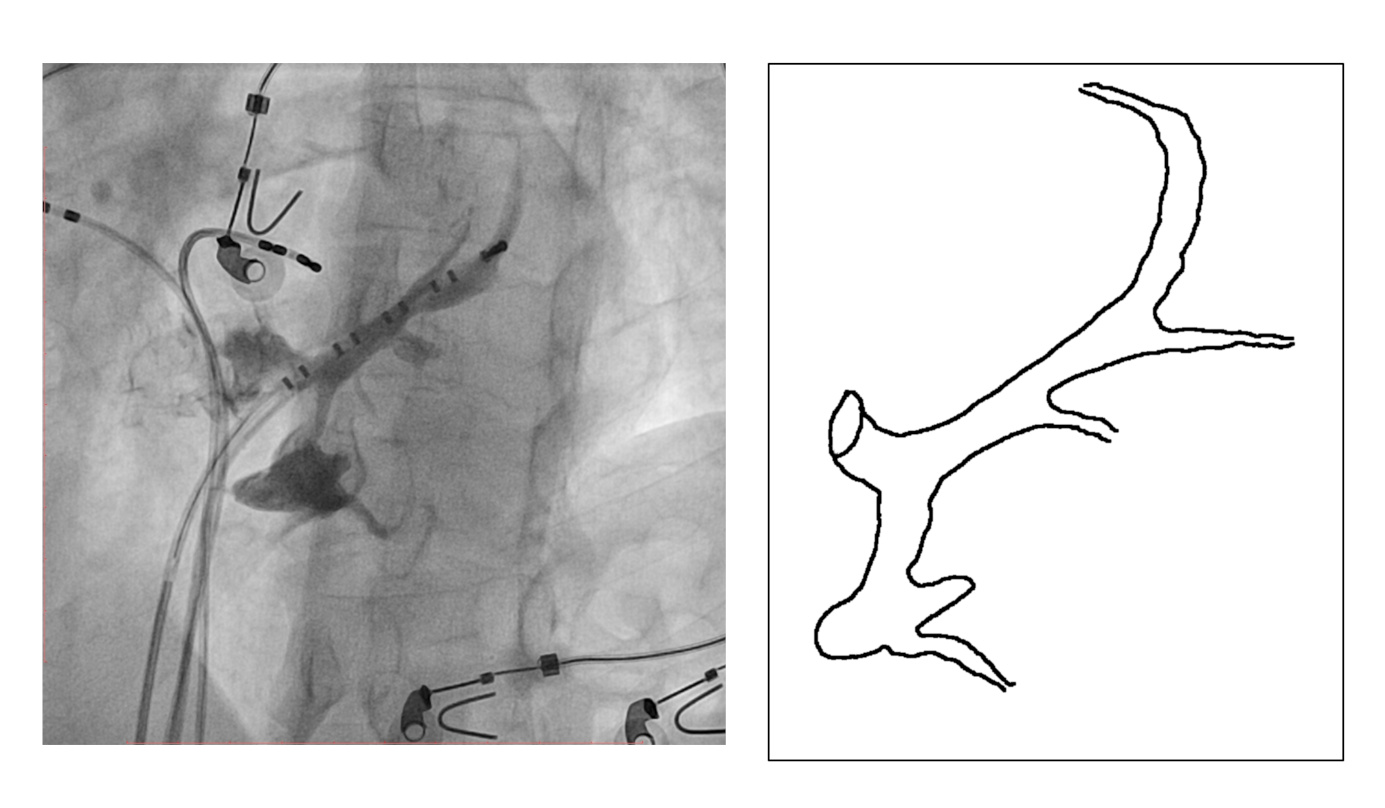
Mapping in diverticulum
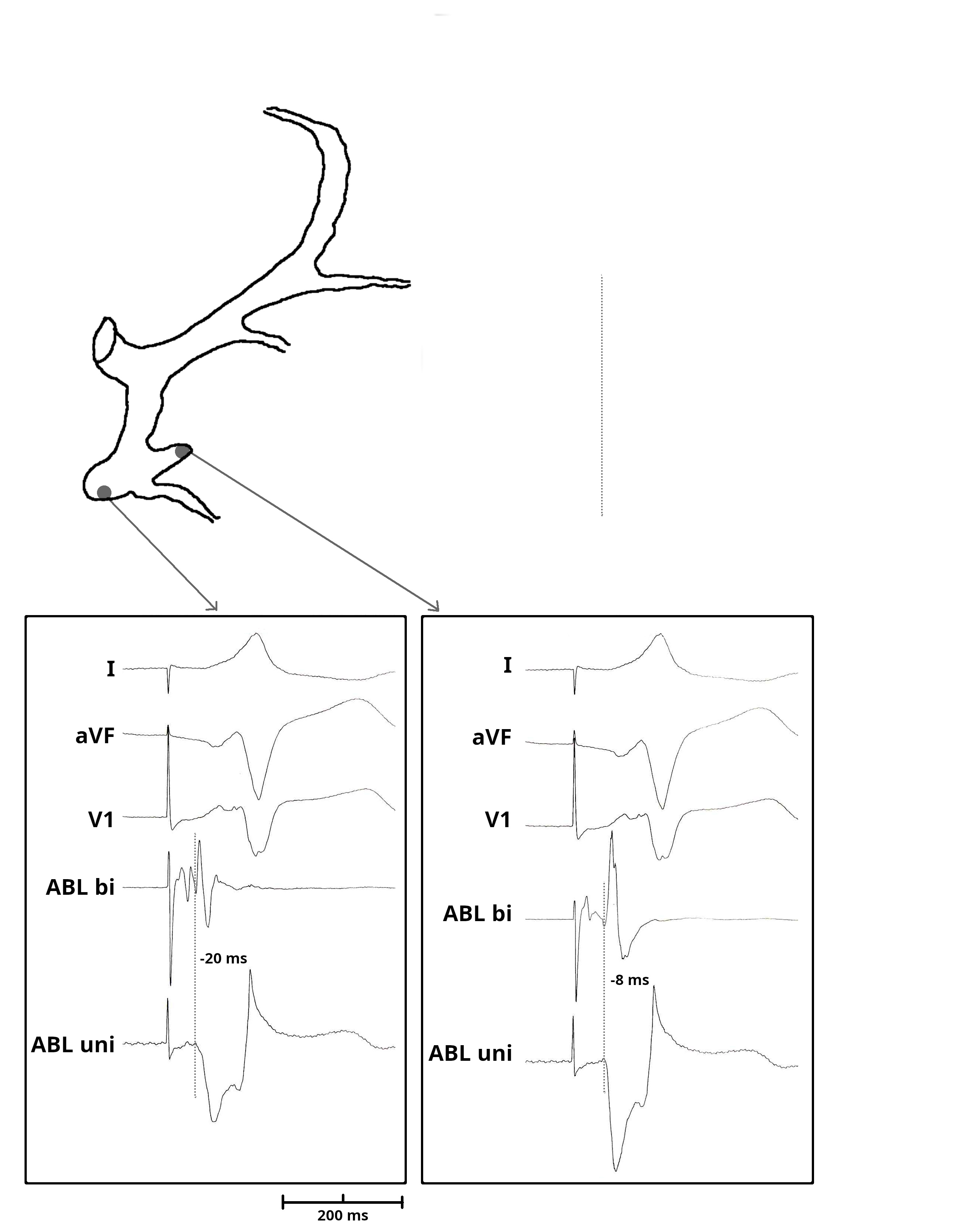
Mapping in diverticulum
Mapping in diverticulum - CSE potential most important
Selvaraj RJ et al. Radiofrequency ablation of posteroseptal accessory pathways associated with coronary sinus diverticula. J Interv Card Electrophysiol. 2016 Nov;47(2):253-259. doi: 10.1007/s10840-016-0113-x.
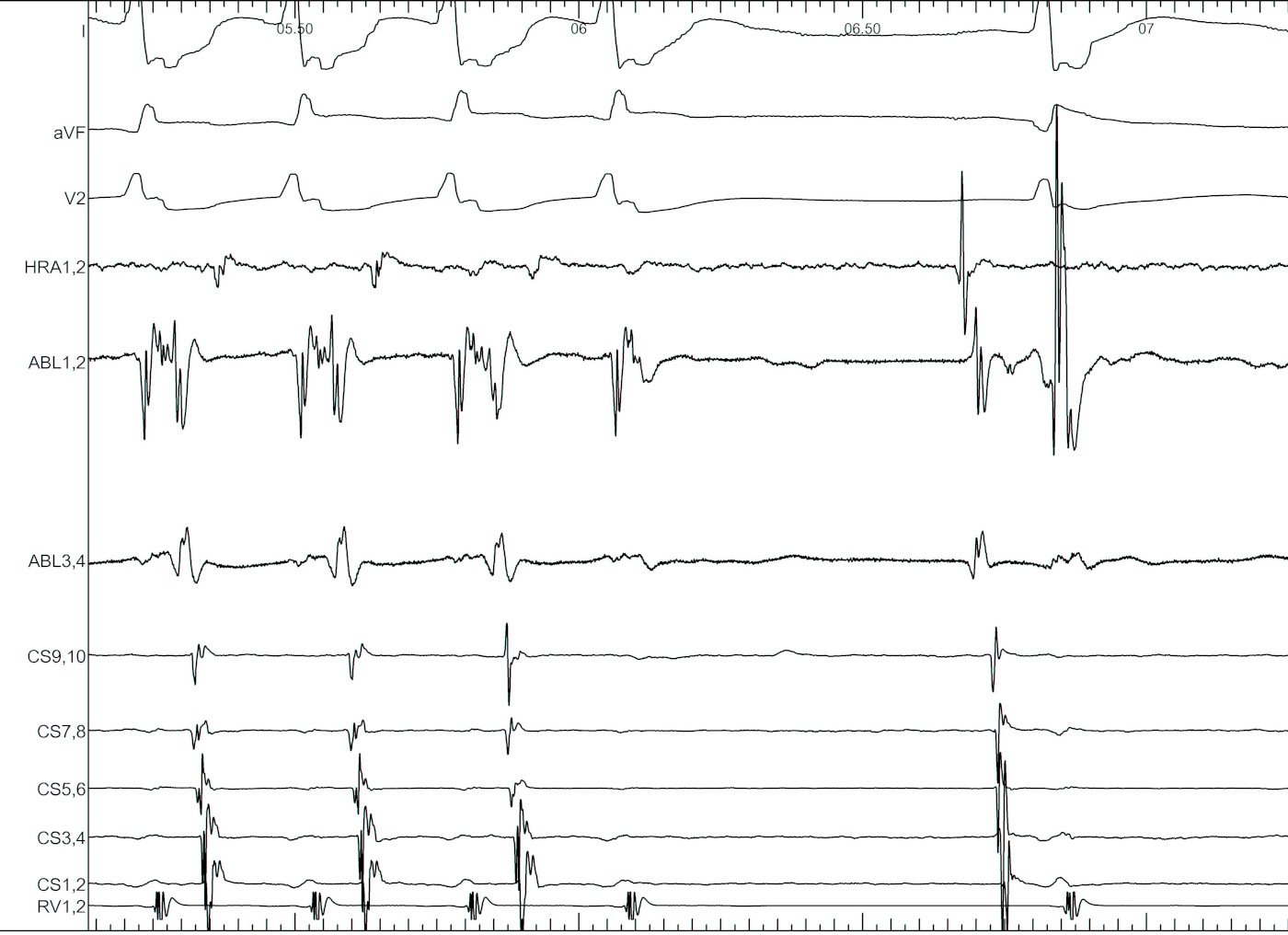
In absence of diverticulum, map along tributaries
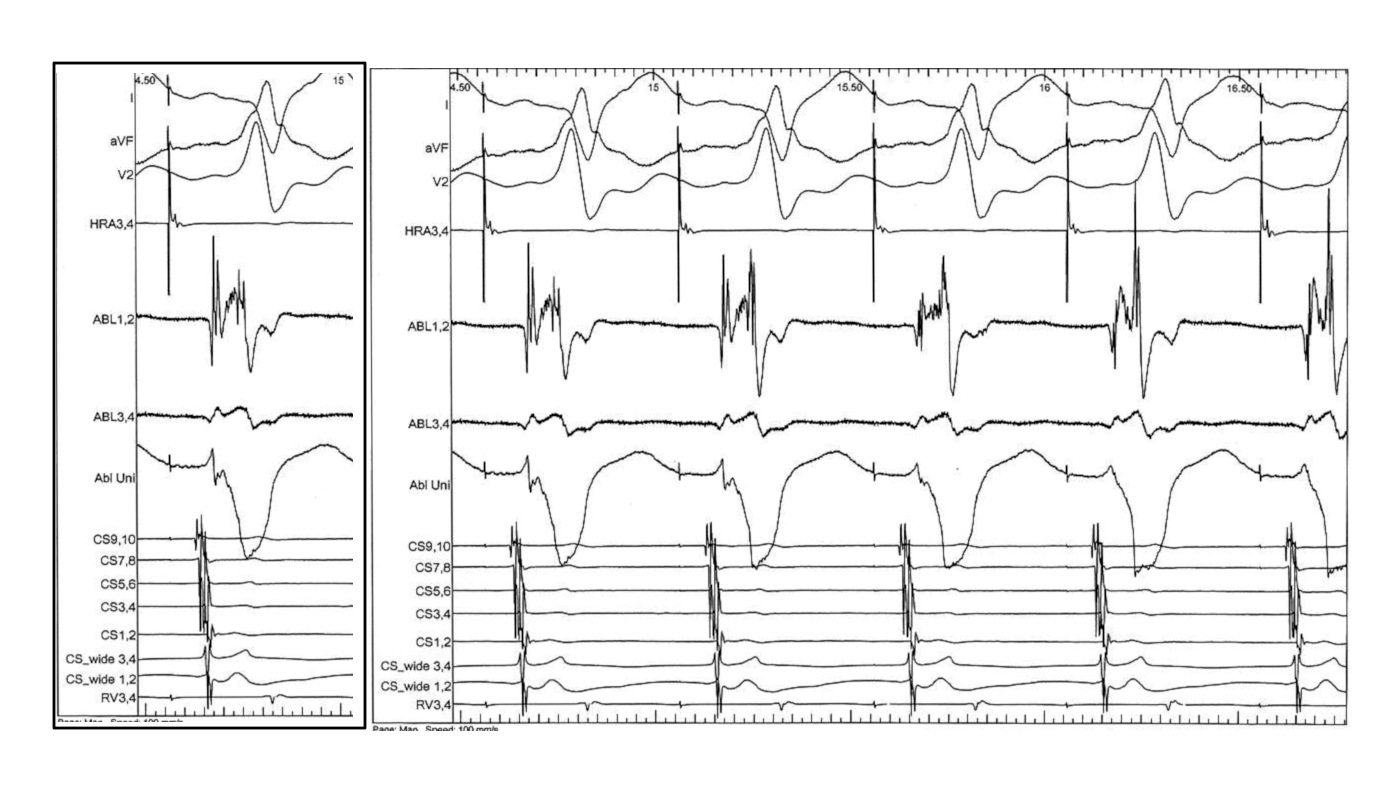
AP slant - Earliest A and earliest V may be distant
AP slant - AP potential more important
Try to avoid bumping, but use it when it happens

Ablation
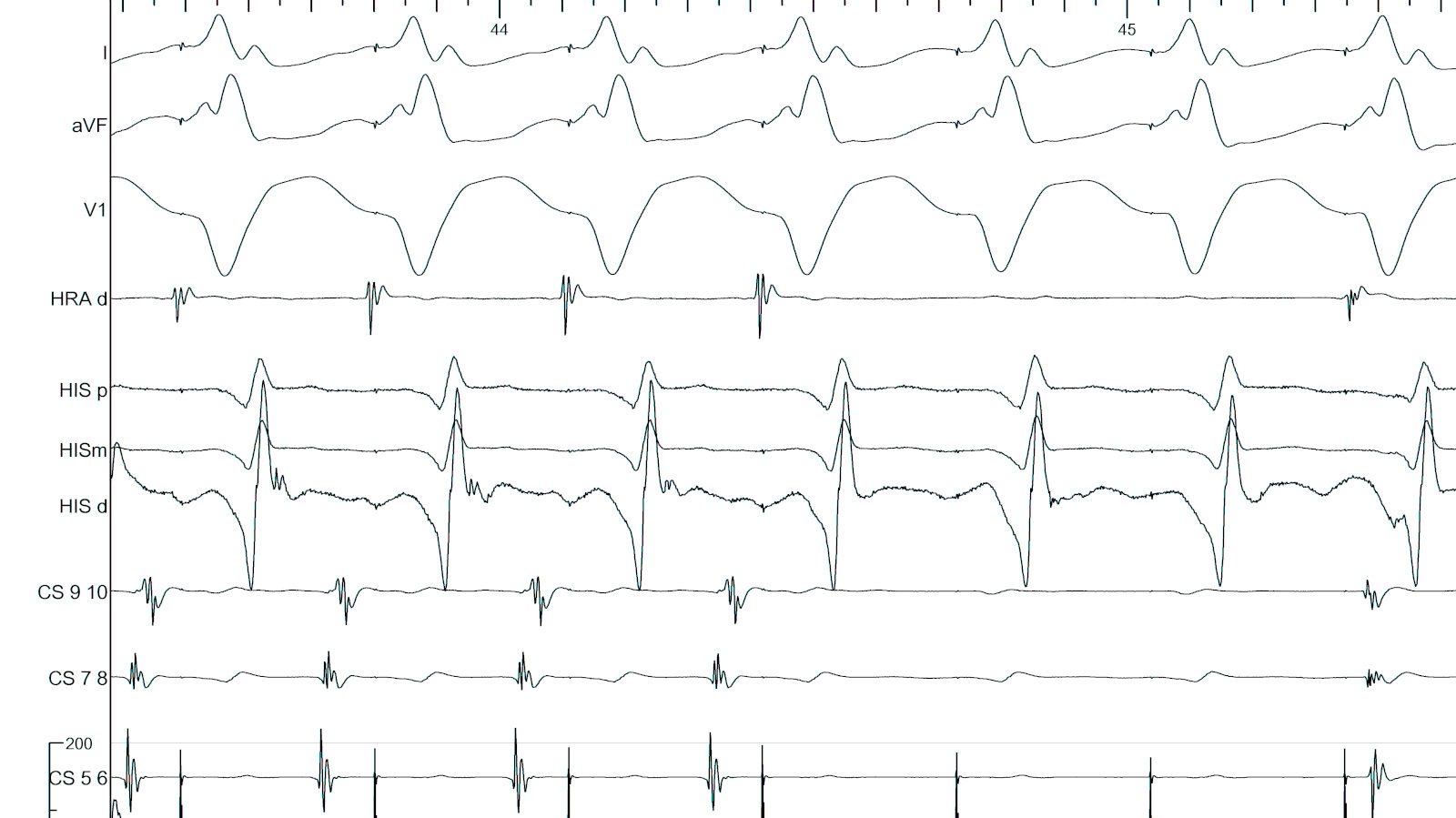
Ablate septal APs during tachycardia when possible
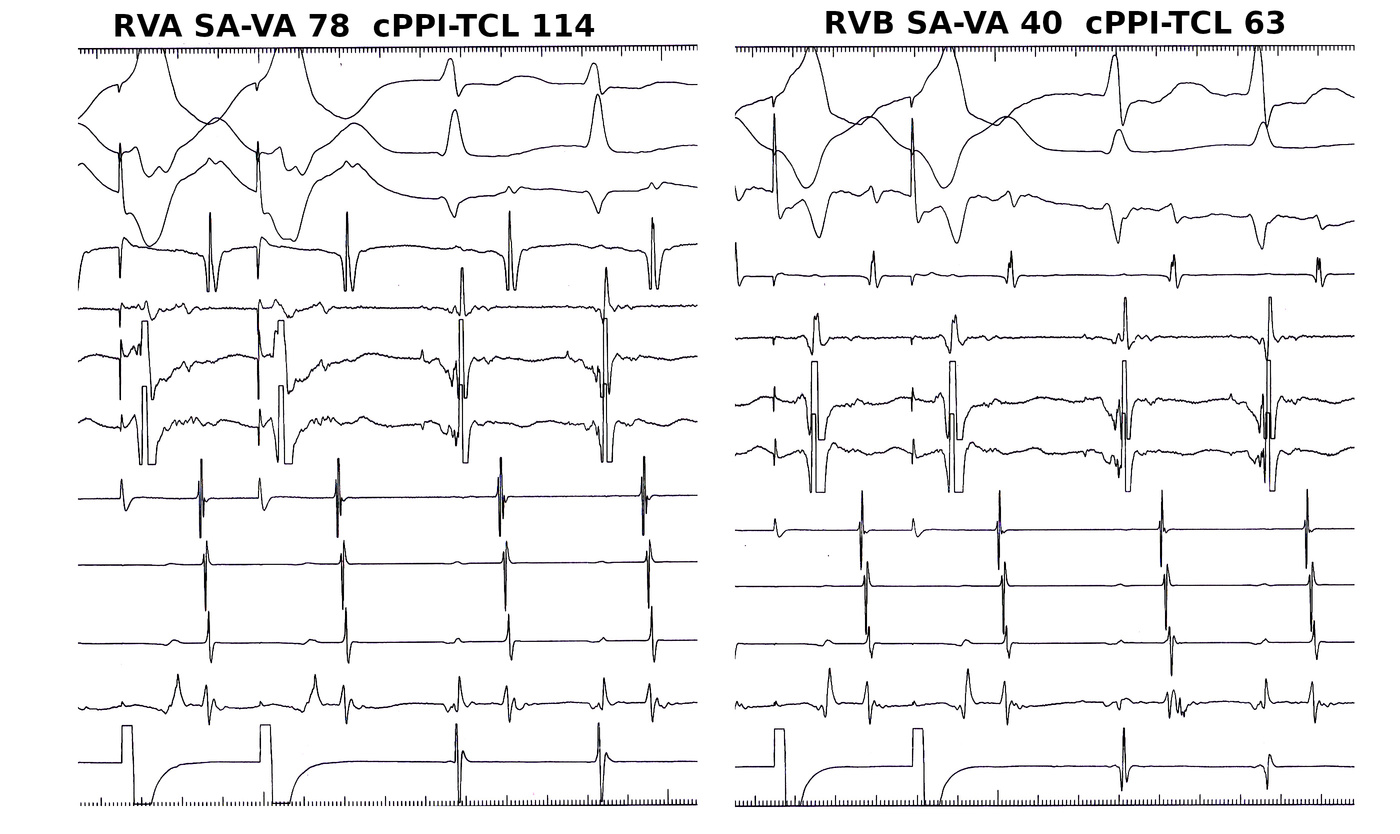
Entrain when ablating free wall AP during tachycardia
Isthmus block
Anteroseptal AP may be ablated from non coronary cusp
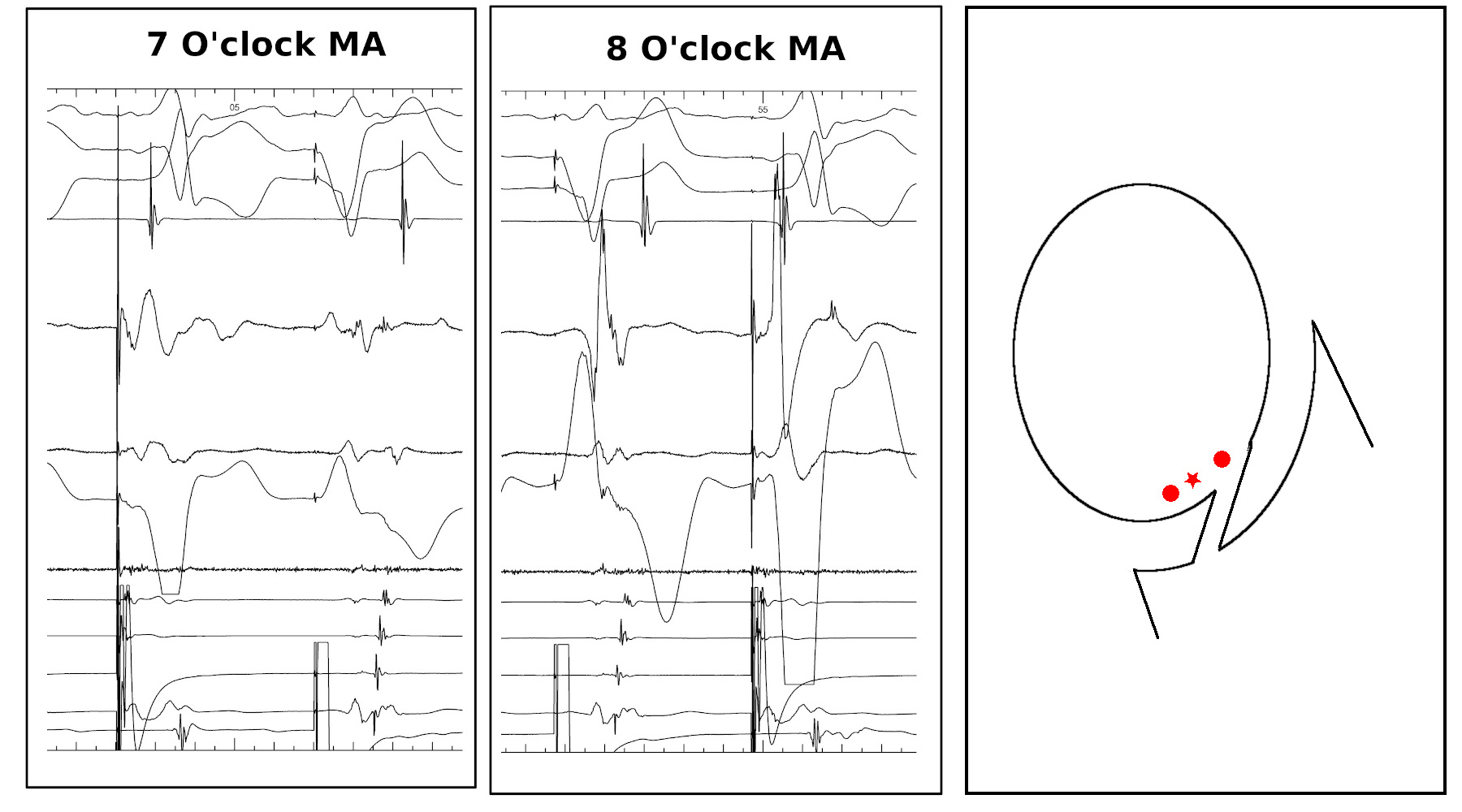
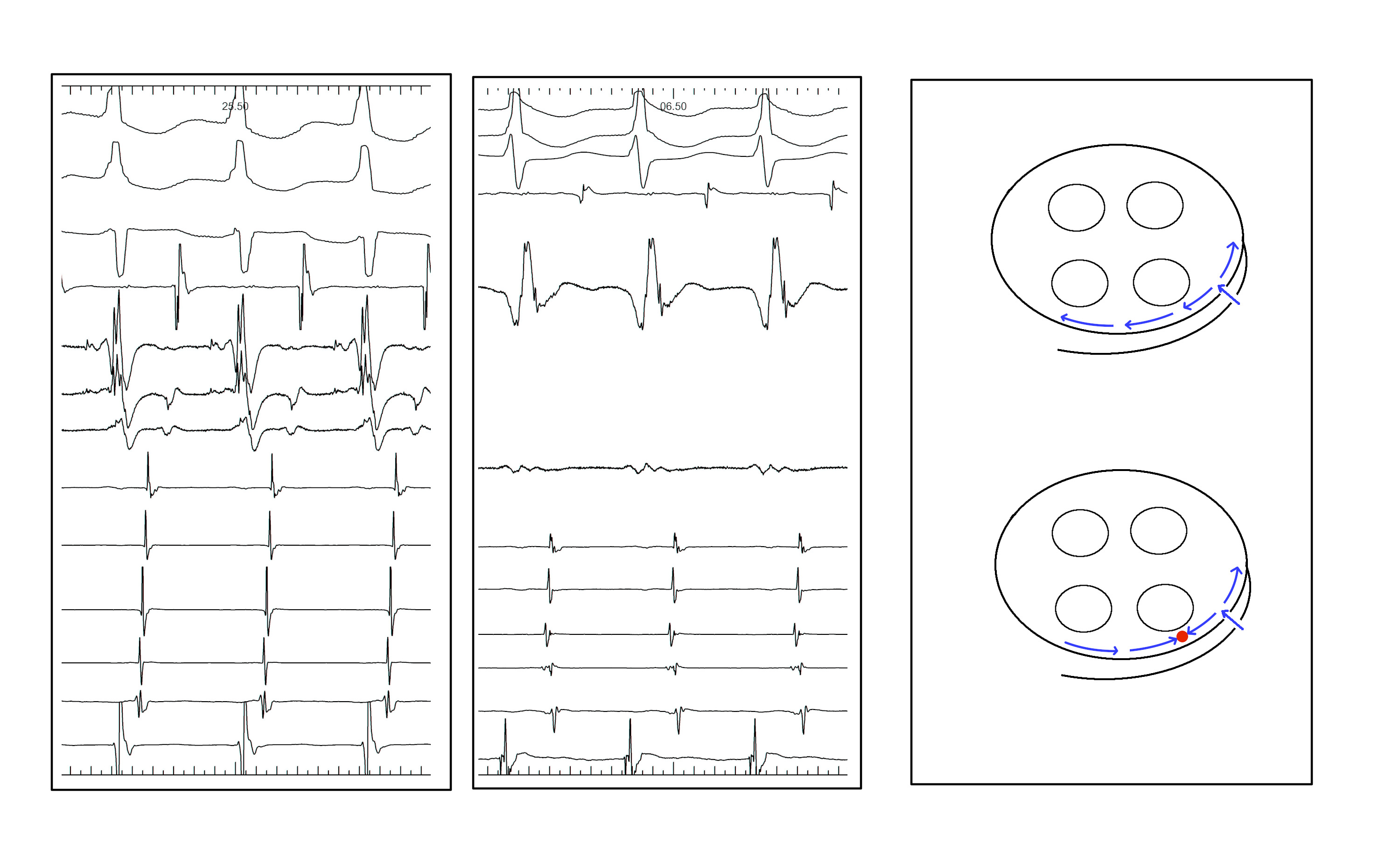
Non annular location of AP
Non annular location of AP
Summary
- Dont make easy ablations difficult
- Accurate diagnosis
- Precise mapping
- Difficult ablations
- Risk of AV injury
- CS diverticulum
- Non annular locations